Hypertensive disorders of pregnancy are a major contributor to maternal morbidity and mortality in the United States and include chronic and gestational hypertension, preeclampsia, HELLP (hemolysis, elevated liver enzymes, and low platelet count) syndrome, eclampsia, and chronic hypertension with superimposed preeclampsia. For patients with chronic hypertension, oral antihypertensive therapy should be initiated or titrated at a blood pressure threshold of 140/90 mm Hg or greater. Gestational hypertension and preeclampsia without severe features can be managed with blood pressure monitoring, laboratory testing for disease progression, antenatal testing for fetal well-being, and delivery at 37 weeks' gestation. The use of antihypertensive drugs to control nonsevere hypertension in the setting of gestational hypertension and preeclampsia does not improve outcomes and is not recommended. Antihypertensive therapy should be initiated expeditiously for acute-onset severe hypertension to prevent hemorrhagic stroke. Preeclampsia with severe features requires immediate stabilization and inpatient treatment with magnesium sulfate for seizure prophylaxis and antenatal corticosteroids (if preterm). Patients in the preterm period should receive antenatal corticosteroids without delaying delivery to complete courses. Hypertensive disorders of pregnancy can worsen or initially present after delivery and account for up to 44% of pregnancy-related deaths in the first six days postpartum. Patients should be monitored closely in the early postpartum period. Hypertensive disorders of pregnancy are linked to poor long-term maternal and fetal outcomes, including increased maternal lifetime risk of cardiovascular disease. Daily low-dose aspirin therapy starting at 12 to 16 weeks' gestation is safe and effective for reducing the risk of preeclampsia for patients with risk factors.
Hypertensive disorders of pregnancy affect 1 in 7 hospital deliveries in the United States, are strongly associated with maternal complications, and account for 7% of pregnancy-related deaths.1–3 Hypertensive disorders of pregnancy, which include chronic hypertension and pregnancy-associated hypertension (gestational hypertension, preeclampsia, HELLP [hemolysis, elevated liver enzymes, and low platelet count] syndrome, eclampsia, chronic hypertension with superimposed preeclampsia), increased in prevalence from 2017 to 2019.1,4 Pregnancy-associated hypertension more than doubles the risk of peripartum coronary disease, cardiomyopathy, and stroke, and accounts for 44% of maternal deaths in the first six days following delivery.4–6
SORT: KEY RECOMMENDATIONS FOR PRACTICE
RCT = randomized controlled trial.
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to https://www.aafp.org/afpsort.
Preeclampsia is a multisystem disease process with pathogenesis involving maternal and placental pathways.2,5 Nonmodifiable risk factors for developing hypertensive disorders of pregnancy include genetic factors; reproductive history, including in vitro fertilization; and certain patient demographics.4,6 Modifiable risk factors for preeclampsia reflect cardiovascular risk and include obesity, dyslipidemia, diabetes mellitus, kidney disease, and chronic hypertension.2,5,7,8 Placental influences begin in early pregnancy with abnormal placentation and spiral artery remodeling, leading to decreased uteroplacental perfusion and oxidative stress.6,7,9,10 Pregnancy, a natural cardiac stress test, can also reveal underlying endothelial dysfunction.6,7
There are significant racial and ethnic disparities in the prevalence of hypertensive disorders of pregnancy. Non-Hispanic Black women have an up to five times higher risk of preeclampsia compared with non-Hispanic White women, are more likely to experience complications from hypertensive disorders of pregnancy, and have a threefold increased risk of inpatient maternal mortality after risk factor adjustment.1,4,11,12 Multiple factors likely contribute to these disparities, including a higher prevalence of risk factors, less access to care, lower-quality care, underrepresentation in research, racial bias in health care, and the physiologic effect of stress from racism.1,5,13–15
Diagnosis
Hypertensive disorders of pregnancy span the entire reproductive period from preconception to postpartum (Figure 1). Chronic hypertension can present before pregnancy, before 20 weeks' gestation, or during pregnancy without resolving postpartum.4,16 Preeclampsia refers to new-onset hypertension after 20 weeks' gestation with proteinuria or end-organ dysfunction. Gestational hypertension describes new-onset hypertension after 20 weeks without proteinuria or end-organ dysfunction. When a patient with gestational hypertension or preeclampsia has severe-range blood pressure (160 mm Hg or greater systolic or 110 mm Hg or greater diastolic on at least two measurements) or end-organ involvement, the diagnosis shifts to preeclampsia with severe features.7 Superimposed preeclampsia is when a person with chronic hypertension has new-onset proteinuria or severe features, including acutely worsening or resistant hypertension. HELLP syndrome is a severe form of preeclampsia that involves hemolysis, liver dysfunction, and thrombocytopenia.7 Table 1 describes diagnostic criteria for hypertensive disorders of pregnancy.4,7,16,17
FIGURE 1.
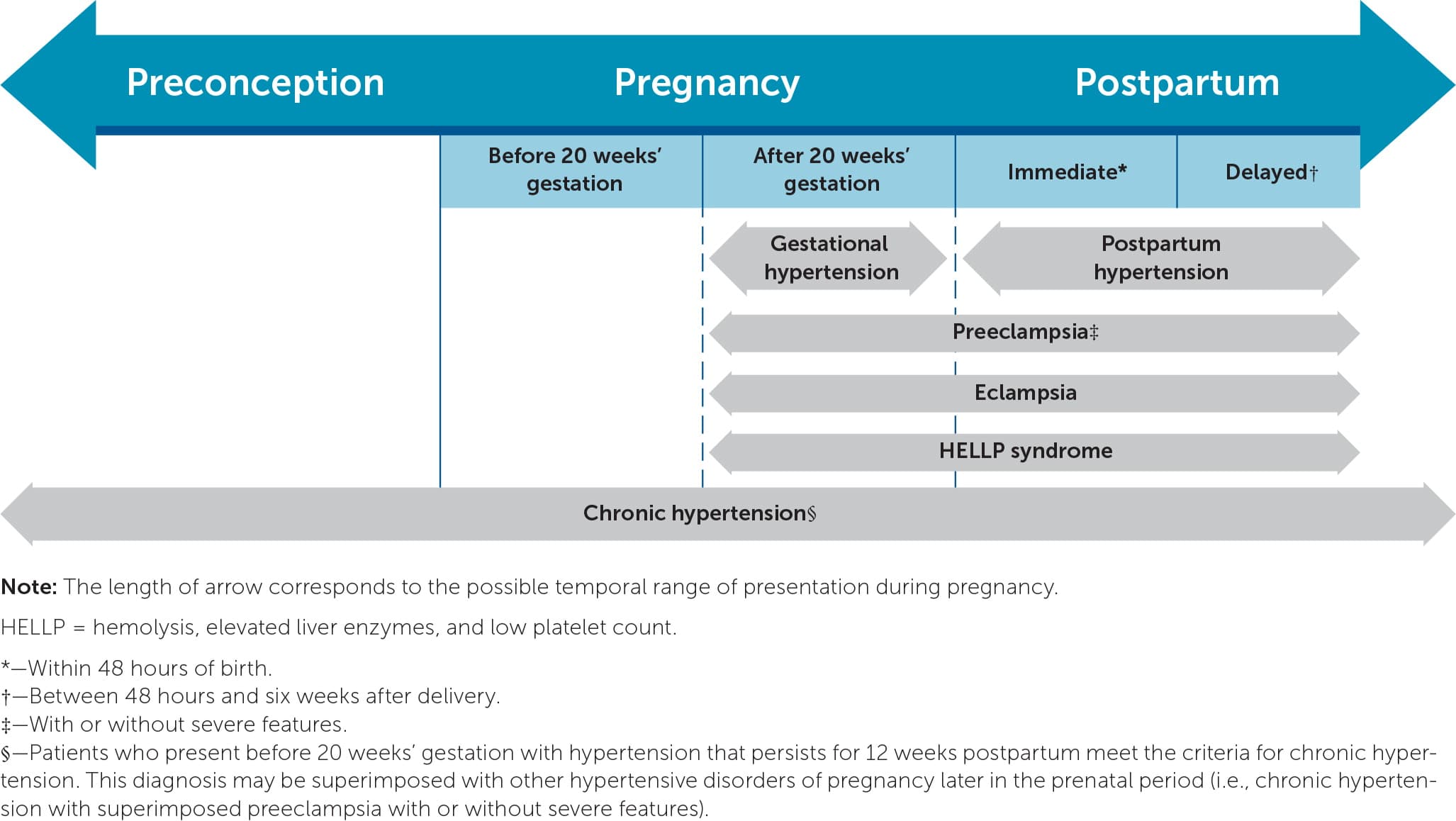
Hypertensive disorders of pregnancy from preconception to postpartum.
TABLE 1. Diagnostic Criteria for Hypertensive Disorders of Pregnancy
| Disorder | Reproductive period | Diagnostic criteria |
|---|---|---|
| Chronic hypertension | Preconception, ≤ 20 weeks' gestation, > 12 weeks postpartum | ≥ 140/90 mm Hg twice at least four hours apart or ≥ 160/110 mm Hg once |
| Gestational hypertension | > 20 weeks' gestation | ≥ 140/90 mm Hg twice at least four hours apart without evidence of proteinuria or severe features |
| Preeclampsia without severe features | > 20 weeks' gestation, postpartum | ≥ 140/90 mm Hg twice at least four hours apart with proteinuria ≥ 300 mg per 24 hours or urine protein/creatinine ratio ≥ 0.3 mg per dL |
| Preeclampsia with severe features | > 20 weeks' gestation, postpartum | Hypertension associated with any of the following: Elevated blood pressure (≥ 160 mm Hg systolic or ≥ 110 mm Hg diastolic) twice at least four hours apart Creatinine > 1.1 mg per dL or > twice baseline Elevated liver function tests (aspartate transaminase or alanine transaminase > twice the upper limit of normal) Platelets < 100 × 103 per μL (100 × 109 per L) Right upper quadrant or epigastric pain New headache Vision changes Pulmonary edema |
| Chronic hypertension with superimposed preeclampsia (with or without severe features) | > 20 weeks' gestation, postpartum | Chronic hypertension with new-onset proteinuria (or a sudden increase in proteinuria if present at baseline) or Development of severe features, including worsening or resistant hypertension (especially acutely) |
| HELLP syndrome | > 20 weeks' gestation, postpartum | Must have all of the following: Hemolysis (elevated lactate dehydrogenase ≥ 600 U per L) Elevated aspartate transaminase or alanine transaminase ≥ twice the upper limit of normal Platelets < 100 × 103 per μL |
| Eclampsia | > 20 weeks' gestation, postpartum | Tonic-clonic, focal, or multifocal seizures |
| Postpartum hypertension | New-onset within six weeks after delivery | ≥ 140/90 mm Hg twice at least four hours apart Immediate: if hypertension occurs within 48 hours after delivery Delayed: if hypertension occurs betwe |
HELLP = hemolysis, elevated liver enzymes, and low platelet count.
*—Seizures can occur without hypertension or severe features of preeclampsia and with a normal blood pressure.
CHRONIC HYPERTENSION
The diagnostic threshold for hypertension in pregnancy is a systolic blood pressure of 140 mm Hg or greater or a diastolic blood pressure of 90 mm Hg or greater on two measurements at least four hours apart. Severe-range blood pressure quickly confirms the diagnosis, and treatment should be expedited.4 One study found that pregnant women with a systolic blood pressure of 130 to 139 mm Hg or diastolic blood pressure of 80 to 89 mm Hg are at greater risk of gestational diabetes, preterm birth, and infant neonatal intensive care admissions compared with those who have normal blood pressure.18,19 Although 20 weeks' gestation is conventionally used to distinguish chronic from gestational hypertension, a retrospective study found that 39% of patients with normal blood pressure before pregnancy developed hypertension without proteinuria before 20 weeks that resolved postpartum. Of patients with chronic hypertension, up to 50% develop superimposed preeclampsia.4,11
GESTATIONAL HYPERTENSION AND PREECLAMPSIA
Pregnancy-associated hypertension represents a spectrum of illnesses that have an onset after 20 weeks' gestation. Screening recommendations focus on blood pressure monitoring during pregnancy.20 Biomarkers and uterine artery Doppler ultrasonography have limited use in predicting preeclampsia.2,7 Gestational hypertension with severe-range blood pressure has the same risk as preeclampsia with severe features and should be treated accordingly.4 Up to one-half of women with gestational hy pertension develop preeclampsia, and the risk is higher when gestational hypertension presents before 32 weeks.7
HELLP SYNDROME
HELLP syndrome is a severe form of preeclampsia associated with high morbidity and mortality. Malaise and right upper quadrant pain occur in 90% of patients with HELLP. Rapid clinical deterioration is a characteristic of HELLP. All components of the diagnostic criteria are necessary and distinguish HELLP from conditions such as preeclampsia complicated by disseminated intravascular coagulation, acute fatty liver disease of pregnancy, or thrombotic thrombocytopenic purpura. Additionally, 15% of patients with HELLP do not have hypertension or proteinuria, and up to one-third present in the postpartum period.7,21
ECLAMPSIA
Eclampsia is a new-onset tonic-clonic, focal, or multifocal seizure in a pregnant or postpartum patient with a hypertensive disorder of pregnancy and without an alternative diagnosis for seizure. Eclampsia is a primary cause of maternal death globally.7 One-half of eclampsia cases present before labor, with the other half presenting in the intrapartum or postpartum period. Eclamptic seizures can occur without warning; however, 80% are preceded by neurologic symptoms, including headaches, visual disturbances, and altered cognition.22
POSTPARTUM HYPERTENSION
Although preeclampsia typically begins to resolve after delivery, patients can experience significant hypertension-related morbidity and mortality postpartum, especially in the first 48 hours following delivery. Postpartum hypertension is most common in patients with hypertension during pregnancy but can develop as new-onset hypertension or preeclampsia up to six weeks after delivery.7,17 Notably, 1 in 5 eclamptic seizures initially presents postpartum, and 15% occur before preeclampsia is recognized.22
Evaluation and Management
Evaluation and management of hypertensive disorders of pregnancy are summarized in Table 2.4,7,11,16,23–27
TABLE 2. Evaluation and Management of Hypertensive Disorders of Pregnancy
| Disorder | Evaluation | Blood pressure treatment | Antenatal surveillance | Timing of delivery | Other considerations |
|---|---|---|---|---|---|
| Chronic hypertension | Baseline CBC, BUN, serum creatinine, electrolytes, aspartate transaminase/alanine transaminase, urine protein/creatinine, electrocardiography or echocardiography (as indicated) | Initiate or titrate medication if blood pressure ≥ 140/90 mm Hg | Third-trimester growth ultrasonography | Controlled, not requiring medication: 38 weeks 0 days' to 39 weeks 6 days' gestation Controlled, on medication: 37 weeks 0 days' to 39 weeks 6 days' gestation | — |
| Gestational hypertension | Initial: CBC, serum creatinine, aspartate transaminase/alanine transaminase, LDH, urine protein/creatinine After diagnosis: office blood pressure measurement one or two times per week Weekly tests: CBC, serum creatinine, aspartate transaminase/alanine transaminase, urine protein/creatinine | No | Growth ultrasonography every three to four weeks Nonstress test, biophysical profile or modified biophysical profile one or two times per week Weekly amniotic fluid assessment | 37 weeks 0 days' gestation or at diagnosis if diagnosed later | For severe features or sustained blood pressure ≥ 160/110 mm Hg, then diagnose and manage as preeclampsia with severe features |
| Preeclampsia (including superimposed) without severe features | Initial: CBC, serum creatinine, aspartate transaminase/alanine transaminase, LDH, urine protein/creatinine After diagnosis: office blood pressure measurement one or two times per week Weekly tests: CBC, serum creatinine, aspartate transaminase/alanine transaminase | No | Growth ultrasonography every three to four weeks Nonstress test, biophysical profile, or modified biophysical profile one to two times per week Weekly amniotic fluid assessment | 37 weeks 0 days' gestation or at diagnosis if diagnosed later | — |
| Preeclampsia (including superimposed) with severe features | Initial: CBC, serum creatinine, aspartate transaminase/alanine transaminase, LDH, urine protein/creatinine Inpatient management from diagnosis until after delivery | Initiate or titrate medications if blood pressure ≥ 160/110 mm Hg | Growth ultrasonography every three to four weeks Inpatient antenatal surveillance with daily non-stress tests from diagnosis | 34 weeks 0 days' gestation or at diagnosis if diagnosed later (earlier if contraindication to expectant management) | Seizure prophylaxis (magnesium sulfate) Antenatal corticosteroids if < 34 weeks' gestation 34 weeks 0 days' to 36 weeks 6 days' gestation if candidate for late-preterm steroids |
| HELLP syndrome | Initial: CBC, BUN, serum creatinine, aspartate transaminase/alanine transaminase, LDH, urine protein/creatinine Inpatient management from diagnosis until after delivery | Initiate or titrate medications if blood pressure ≥ 160/110 mm Hg | Inpatient monitoring | Plan for delivery after maternal stabilization (via induction of labor or cesarean delivery) | Seizure prophylaxis (magnesium sulfate) Antenatal corticosteroids < 34 weeks' gestation 34 weeks 0 days' to 36 weeks 6 days' gestation if candidate for late-preterm steroids |
| Eclampsia | Inpatient management from diagnosis until after delivery | Initiate or titrate medications if blood pressure > 160/110 mm Hg | Inpatient monitoring | Plan for delivery after maternal stabilization (via induction of labor or cesarean delivery) | Treat seizures with magnesium sulfate Airway protection, prevent maternal injury |
| Postpartum hypertension | If new onset, check CBC, serum creatinine, aspartate transaminase/alanine transaminase, LDH, urine protein/creatinine to evaluate for postpartum preeclampsia | Threshold to initiate oral antihypertensive medications ≥ 150/100 mm Hg | — | — | Seizure prophylaxis (magnesium sulfate) if new-onset postpartum preeclampsia with severe features |
BUN = blood urea nitrogen; CBC = complete blood count; HELLP = hemolysis, elevated liver enzymes, and low platelet count; LDH = lactate dehydrogenase.
CHRONIC HYPERTENSION
When hypertension is diagnosed before 20 weeks' gestation, cardiac function is a primary concern. Patients with long-standing hypertension (typically 10 years or longer but depends on severity and age at onset) are at risk of heart disease, including hypertrophy, cardiomegaly, and ischemic disease. Clinical evaluation includes a cardiovascular examination for potential cardiac dysfunction. Electrocardiography is recommended for patients older than 30 years and those with at least four years of poorly controlled disease. Echocardiography is warranted if electrocardiography findings are abnormal.4 A baseline laboratory evaluation at the initial prenatal visit or after diagnosis should include a urine protein/creatinine ratio or 24-hour urine protein measurement, complete blood count, and serum creatinine, blood urea nitrogen, serum potassium, aspartate transaminase, and alanine transaminase testing.4
Oral antihypertensive therapy should be initiated or titrated when blood pressure is 140/90 mm Hg or greater. A treatment threshold of 140/90 mm Hg reduces adverse pregnancy outcomes compared with 160/105 mm Hg (number needed to treat [NNT] = 15; 95% CI, 9.4 to 33.7) without affecting fetal growth.11 Treatment for a systolic blood pressure of 130 to 139 mm Hg or diastolic blood pressure of 80 to 89 mm Hg may be appropriate when patients have underlying cardiovascular comorbidities.4 Labetalol and extended-release nifedipine are first-line oral medications for chronic hypertension in pregnancy.4,11 Angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers should be avoided because of their teratogenic effects. Thiazide diuretics may be continued when used before pregnancy and can be added as second-or third-line medications (Table 3).4,16
TABLE 3. Pharmacologic Management of Hypertension During Pregnancy
| Medication | Dosage | Frequency | Comments |
|---|---|---|---|
| Treatment of chronic hypertension | |||
| Labetalol (first-line) | 200 to 2,400 mg per day orally | Divided doses every 8 to 12 hours | Avoid with uncontrolled asthma, cardiomyopathy |
| Nifedipine, extended-release (first-line) | 30 to 120 mg per day orally | Once daily | May cause tachycardia |
| Methyldopa | 250 to 3,000 mg per day orally | Divided doses every 6 to 12 hours | May be less effective; may cause sedation |
| Hydrochlorothiazide | 12.5 to 25 mg per day orally | Once daily | May cause dehydration, electrolyte abnormalities |
| Rapid treatment of severe persistent hypertension | |||
| Nifedipine, immediate-release | Starting dose: 10 mg orally Increase to 20 mg for up to 2 more doses | 20-minute intervals | Transition to labetalol or hydralazine if still severe |
| Labetalol | Starting dose: 20 mg intravenously Increase to 40 mg then 80 mg if still severe (maximum cumulative dose = 300 mg) | 10-minute intervals | Transition to hydralazine or oral nifedipine if still severe |
| Hydralazine | Starting dose: 5 mg intravenously Give additional 5 to 10 mg (maximum cumulative dose = 20 mg) | 20-minute intervals | Transition to labetalol or oral nifedipine if still severe |
Chronic hypertension is associated with fetal growth restriction, and thus third-trimester ultrasonography is recommended. 4 Subsequent ultrasonography may be recommended based on the initial growth assessment. Antenatal fetal testing with a nonstress test, biophysical profile, or modified biophysical profile, including a nonstress test and an assessment of amniotic fluid volume, is recommended for patients with chronic hypertension requiring medications or associated with conditions affecting fetal outcomes.3,23 For patients with chronic hypertension requiring medications, weekly antenatal testing starting at 32 weeks' gestation is recommended.23 Timing of delivery should be based on a balance of maternal, fetal, and neonatal risks and range from 37 to 39 weeks' gestation for uncomplicated chronic hypertension.4,16
GESTATIONAL HYPERTENSION AND PREECLAMPSIA WITHOUT SEVERE FEATURES
After the initial diagnosis, the evaluation for patients with gestational hypertension and preeclampsia without severe features includes at least weekly office visits with blood pressure monitoring, symptom assessment, urine protein measurement to assess for preeclampsia, and laboratory evaluation to assess for severe features.7 Although there are limited data for the timing and interval of antenatal fetal surveillance, testing is recommended because of the risk of fetal growth restriction and death. The American College of Obstetricians and Gynecologists suggests fetal testing once or twice per week and weekly assessment of amniotic fluid volume.7,23 Growth ultrasonography is recommended at diagnosis and every three to four weeks. In contrast with chronic hypertension, the use of antihypertensive drugs for nonsevere hypertension does not alter disease progression or improve outcomes and is not recommended.7 Delivery is recommended at 37 weeks' gestation or at the time of diagnosis if after 37 weeks.7,24
PREECLAMPSIA WITH SEVERE FEATURES
Preeclampsia with severe features is associated with significant morbidity and rapid disease progression, and inpatient management is required from diagnosis until after delivery. When severe features are diagnosed at 34 weeks' gestation or later, delivery is recommended after maternal stabilization.7 If severe features are diagnosed before 34 weeks' gestation, inpatient expectant management can be considered with serial maternal and fetal surveillance to delay delivery to 34 weeks. Progression to delivery is recommended if maternal or fetal status deteriorates7,24 (Table 47 ).
TABLE 4. Indications for Expeditious Delivery in Preeclampsia With Severe Features at Less Than 34 Weeks' Gestation
| Maternal |
| Abruptio placentae |
| Disseminated intravascular coagulation |
| Eclampsia |
| HELLP syndrome |
| Myocardial infarction |
| Persistent severe symptoms (neurologic or gastrointestinal) |
| Pulmonary edema |
| Renal insufficiency |
| Stroke |
| Fetal |
| Abnormal fetal testing |
| Fetal death |
| Lethal anomaly or extreme prematurity |
| Reverse end-diastolic flow on umbilical artery Dopplers |
Note: In patients who have preeclampsia with severe features at 34 weeks' gestation or more, delivery is recommended after maternal stabilization.
HELLP = hemolysis, elevated liver enzymes, and low platelet count.
Information from reference 7.
Due to the risk of cardiac events, renal injury, and ischemic or hemorrhagic stroke, antihypertensive therapy should be initiated within 30 to 60 minutes if acute-onset severe hypertension persists for 15 minutes.4,7 First-line treatments for acute severe hypertension include intravenous labetalol, intravenous hydralazine, and oral immediate-release nifedipine, which is particularly useful when intravenous access has not been established7 (Table 34,16 ).
Magnesium sulfate helps prevent eclamptic seizures (NNT = 100) and placental abruption (NNT = 100) in preeclampsia with severe features.25 For patients who have preeclampsia with severe features, intravenous magnesium sulfate is initiated with a loading dose of 4 to 6 g followed by a maintenance infusion of 1 to 2 g per hour. Close monitoring of respiratory status, urine output, mental status, and reflexes is required to assess for potential magnesium toxicity.7,24 Early signs of toxicity include the loss of deep tendon reflexes, and severe toxicity can present with respiratory depression, apnea, and cardiac arrest.7,24,25
HELLP SYNDROME
For patients with HELLP syndrome, delivery at a tertiary care center is recommended at the time of diagnosis.7,21 Just as magnesium sulfate is used for preeclampsia with severe features, it should be initiated for seizure prophylaxis.24 A Cochrane review including limited studies of high-dose steroids found that they were not beneficial for HELLP syndrome.28 Laboratory testing (complete blood count, lactate dehydrogenase, blood urea nitrogen, creatinine, aspartate transaminase, alanine transaminase) should be performed at least every 12 hours and continued postpartum until levels improve or stabilize.7
ECLAMPSIA
Treatment of eclampsia includes protecting the maternal airway, avoiding injury, and promptly initiating magnesium sulfate. Compared with other anticonvulsants, magnesium sulfate is more effective for treating eclamptic seizures, preventing recurrent seizures, and decreasing mortality. The addition of other medications is not beneficial. For patients who received a loading dose of magnesium sulfate for prophylaxis, an additional 2-4 g bolus should be administered after a seizure. [corrected] For other patients, a loading dose of 4 to 6 g should be administered over 20 minutes.7,25
Mode of Delivery
Vaginal delivery is preferred for patients with chronic hypertension, gestational hypertension, and preeclampsia without severe features in the absence of specific indications for cesarean delivery.7 For patients who have preeclampsia with severe features, induction of labor is a reasonable option; however, cesarean delivery rates of up to 97% for patients less than 28 weeks' gestation and 65% for patients 28 to 32 weeks' gestation have been reported. Decisions about the mode of delivery for patients remote from term should be individualized based on gestational age, disease progression, and fetal status.7 Although antenatal corticosteroids are recommended before 34 weeks' gestation and can be considered before 37 weeks, in preeclampsia with severe features, delivery should not be delayed to complete steroid administration.26,27
Postpartum Care
After delivery, most people with preeclampsia experience diuresis, lower blood pressure, and general improvement. Magnesium sulfate should be continued for 24 hours postpartum. Hypertension may worsen while third-space fluid returns to the vasculature and can peak three to six days postpartum.17,29 Close monitoring and outpatient follow-up within the first seven to 10 days is recommended for patients with gestational hypertension or preeclampsia.29 Home blood pressure monitoring may increase the likelihood of obtaining blood pressure measurements at the recommended time, reduce hypertension-related hospital readmissions, and narrow disparities in adherence to postpartum follow-up.30
Antihypertensive medications administered postpartum should be started or titrated to maintain a systolic blood pressure of less than 150 mm Hg and a diastolic blood pressure of less than 100 mm Hg to prevent the development of severe hypertension.24,31 Antihypertensive medications are safe during lactation, although thiazides may decrease milk volume.4,16,17 Treatment of acute-onset severe hypertension follows the same protocols after delivery7 (Table 34,16 ). All postpartum patients should receive information about hypertensive warning signs before discharge.7,17
Prevention
Aspirin therapy is a safe and effective risk-reduction strategy in patients with risk factors for developing preeclampsia5,8,32,33 (Table 534 ). In these patients, daily low-dose aspirin (81 mg) lowers the likelihood of developing preeclampsia by 15% and decreases the risk of preterm birth, small-for-gestational-age infants, and perinatal mortality.5,8,35 Aspirin should be initiated after 12 weeks' gestation (optimally before 16 weeks) and continued until delivery.5,7 Calcium supplementation may decrease the risk of preeclampsia, particularly for patients with low-calcium diets; however, high-quality evidence is lacking.9,33
TABLE 5. Risk Assessment for Preeclampsia
| Risk level | Risk factors* | Recommendation |
|---|---|---|
| High† | History of preeclampsia, especially when accompanied by an adverse outcome Multifetal gestation Chronic hypertension Pregestational type 1 or 2 diabetes mellitus Kidney disease Autoimmune disease (systemic lupus erythematosus, anti-phospholipid syndrome) Combination of multiple moderate-risk factors | Recommend low-dose aspirin if the patient has one or more high-risk factors |
| Moderate‡ | Nulliparity Obesity (body mass index > 30 kg per m2) Family history of pre-eclampsia (mother or sister) Black race (due to social, rather than biologic, factors)§ Lower income§ Age 35 years or older Personal history factors (e.g., low-birth-weight or small-for-gestational-age infant, previous adverse pregnancy outcome, > 10-year pregnancy interval) In vitro conception | Recommend low-dose aspirin if the patient has two or more moderate-risk factors Consider low-dose aspirin if the patient has one moderate-risk factor |
| Low | Prior uncomplicated term delivery without risk factors | Do not recommend low-dose aspirin |
*—Includes only risk factors obtained from the patient's medical history. Clinical measures are not included.
†—High-risk factors are associated with the greatest risk of preeclampsia. Preeclampsia incidence rate would be approximately 8% or greater in a pregnant person with one or more high-risk factors.
‡—Moderate-risk factors are independently associated with preeclampsia.
§—Factors associated with increased risk due to environmental, social, and historical inequities shaping health exposures, access to health care, and unequal resource allocation, not biologic propensities.
Adapted from U.S. Preventive Services Task Force. Aspirin use to prevent preeclampsia and related morbidity and mortality: preventive medication. September 28, 2021. Accessed January 8, 2024. https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/low-dose-aspirin-use-for-the-prevention-of-morbidity-and-mortality-from-preeclampsia-preventive-medication.
Prognosis
Hypertensive disorders of pregnancy are associated with short- and long-term maternal and fetal complications.2,5–7,11,16,36,37 There is also a risk of recurrence in subsequent pregnancies.36,37 Fetal and neonatal complications include low-birth-weight infants, preterm delivery, perinatal mortality, congenital malformations, and cognitive issues in childhood and beyond.5,16,37 Studies suggest there is an increased risk of hypertension, obesity, and cardiovascular disease (CVD) in infants that extends into adulthood.6
People who have had hypertensive disorders of pregnancy have twice the risk of CVD throughout their lifetime compared with patients who have not, and an increased risk of stroke, heart failure, and kidney disease.5,7,11,36–38 Patients with pregnancy-associated hypertension have a fivefold greater lifetime risk of hypertension and are diagnosed an average of 10 years younger than patients without pregnancy-associated hypertension.2,7 These risks are higher with recurrent preeclampsia or more severe manifestations.7,16,38 One explanation is that underlying endothelial dysfunction predisposes patients to hypertensive disorders of pregnancy and CVD. Physiologic stress of pregnancy and cardiovascular changes associated with hypertensive disorders of pregnancy may cause cellular remodeling that contributes to future CVD.2
Postpartum counseling should emphasize the importance of ongoing primary care because of the risk of future CVD. Regular health care visits should include blood pressure monitoring, the evaluation for and treatment of comorbidities such as high cholesterol, diabetes, and tobacco use, and ongoing education about a healthy lifestyle (e.g., stress reduction, sleep hygiene, weight management).37–39
This article updates previous articles on this topic by Leeman, et al.40; Leeman and Fontaine41; Wagner42; and Padden.43
Data Sources: PubMed searches were conducted using the key words hypertensive disorders of pregnancy, hypertension, pregnancy-induced, chronic hypertension in pregnancy, preeclampsia, and eclampsia. We used an evidence summary generated by Essential Evidence Plus with the key words hypertension, pregnancy-induced, preeclampsia, and eclampsia. We searched the Cochrane database and U.S. Preventive Services Task Force recommendations using the key words preeclampsia and hypertensive disorders of pregnancy. The search included meta-analyses, randomized controlled trials, clinical trials, and reviews. Whenever possible, if studies used race or gender as patient categories but did not define how these categories were assigned, they were not included in our final references. If studies that used these categories were determined to be essential and therefore included, limitations were stated or explanations provided in the manuscript. Search dates: December 22, 2022; January 9, 2023; February 20, 2023; and December 28, 2023.
