Seborrheic dermatitis is a common, chronic relapsing skin condition that predominantly affects areas of the body that are rich in sebaceous glands. Clinically, seborrheic dermatitis presents as symmetric, poorly defined erythematous patches with yellow, oily scales and fine, superficial desquamation (flaking). In people who have darker skin, erythema may be less apparent, and postinflammatory pigmentary changes might be a presenting sign with hypopigmented, slightly scaly areas. Seborrheic dermatitis of the scalp can be effectively treated with topical over-the-counter antifungal shampoos and prescription-strength antifungal or corticosteroid solutions, foams, or oils. Thick, scaly areas can be treated with keratolytic shampoos and lotions. Seborrheic dermatitis of the face and body can be treated with over-the-counter and prescription-strength antifungal creams, over-the-counter and prescription-strength corticosteroid creams and ointments, and calcineurin inhibitor cream or ointment. Neonatal seborrheic dermatitis is common and typically self-resolves by 6 months of age. Mild cases of the scalp (cradle cap) may be treated conservatively with mineral oil to loosen scale and gentle combing. More severe cases may overlap with atopic dermatitis and can be treated with topical antifungals or topical corticosteroids.
Seborrheic dermatitis, a common, chronic relapsing skin condition, clinically presents as symmetric, poorly defined erythematous patches with yellow, oily scales and fine, superficial desquamation (flaking).1 Pruritus is a frequent symptom. Commonly affected areas, which are predominantly areas rich in sebaceous glands, include the scalp (colloquially dandruff), face, chest, intertriginous areas (eg, skin folds such as the groin, axillae, and inframammary folds), nasolabial folds, upper eyebrows, and the nasal bridge (Figure 1 and Figure 2).
SORT KEY RECOMMENDATIONS FOR PRACTICE
| Clinical recommendations | Evidence rating | Comments |
|---|---|---|
| Topical antifungal agents are effective in treatment and maintenance of seborrheic dermatitis of the face and scalp.11,13 | A | Multiple randomized controlled trials; Cochrane systematic review |
| Topical anti-inflammatory agents (corticosteroids) are effective in treatment of seborrheic dermatitis of the face or scalp.2,6,13 | A | Multiple randomized controlled trials; Cochrane systematic review |
| Topical calcineurin inhibitors (eg, pimecrolimus 1%, tacrolimus 0.1%), which are safe and effective treatments for seborrheic dermatitis of the face or body, are recommended in cases that are unresponsive to other treatments or to avoid the consequences of long-term corticosteroid use.2,13,14,23–26 | A | Multiple randomized controlled trials |
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to https://www.aafp.org/afpsort.
FIGURE 1.
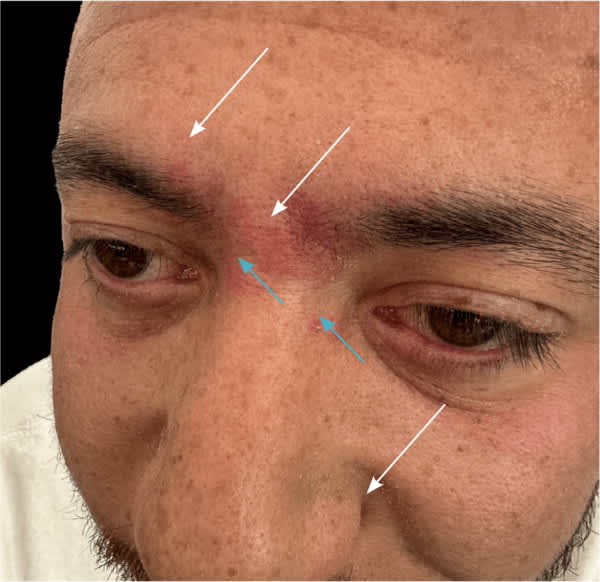
Facial seborrheic dermatitis and rosacea in an adult patient with Fitzpatrick skin type IV. Seborrheic dermatitis is evident in the prominent erythema and fine scaling of the glabella and eyebrows and the lesser erythema and mild scaling on the nasolabial folds (white arrows). The faint, small, pink papules present on the glabella and lateral nasal sidewall (blue arrows) indicate an overlap with rosacea.
FIGURE 2.

Mild to moderate seborrheic dermatitis of an adult with Fitzpatrick skin type II. Note erythema of the eyelid, nasolabial fold, and forehead.
Read the full article
Get immediate access, anytime, anywhere.
Choose a single article, issue, or full-access subscription.
Earn up to 14 CME credits per issue.
