
Family physicians can get paid for common services such as counseling and screenings. The key is recognizing them and knowing how to code them.

Primary care physicians often provide more care than the evaluation and management (E/M) services they typically bill for,1 but many are not familiar enough with the additional services to document and bill for them.
The most common missed opportunities in primary care involve counseling or preventive services, but there are other billable services physicians may be missing out on as well. Once you recognize these services, the key to preventing denials is understanding what diagnosis codes and documentation payers require. Then, you can link the diagnosis codes to the CPT codes in the EHR and make templates to streamline the documentation process.
This article covers several CPT and HCPCS codes for services family physicians often provide but less commonly bill.
KEY POINTS
- Services such as tobacco cessation counseling and intensive behavioral therapy for obesity are appropriate for many patients and can be billed separately from evaluation and management.
- The key to avoiding insurance denials when billing these services is knowing which diagnosis codes to use and how to document your work.
- While the relative value units tied to some of these services may be small, they can add up quickly, and in many cases primary care physicians may already be doing the work and just not billing for it.
BE AWARE: PAYER POLICIES MAY DIFFER
Before we get to the services and codes, first we must note that payer policies for billing these services may differ. Medicare has an online list of covered preventive services with coverage guidelines,2 and Medicare policies will be cited below, where applicable. Commercial payers often follow Medicare policies regarding which ICD-10 codes are associated with which services, but often use different procedure codes. Medicare and Medicare Advantage plans generally use HCPCS codes that start with G (e.g., G0402 for initial preventive physical exams, and G0438 and G0439 for annual wellness visits) while commercial payers use CPT codes (e.g., 99381-99387 and 99391-99397 for annual routine physical exams). When there is no G code or no CPT code for a particular service, then payers will usually cover the other code type.
It’s best to obtain payer policies for each payer you work with on a regular basis. Large practices may have revenue cycle teams or coding teams that can assist with this. You can usually find payer policies by searching online for the specific code and payer or logging into the payer’s provider portal, which will have a list of all the medical policies with reimbursement guidelines.
Another thing worth noting is that, although these are all billable services, they should only be billed when appropriate. If you do not meet the time requirements for a service, you did not complete all required components, or the patient does not need the service, you should not bill for the service. Additionally, it’s important to remember that the patient may have to pay the entire cost of the service if you don’t document or code correctly, because it will be denied. This is why it is important to understand payer guidelines and build documentation and coding requirements into the EHR, if possible. The following guidance should help.
RISK-FACTOR SPECIFIC COUNSELING AND SCREENING SERVICES
Many counseling services are time based, and physicians only need to spend more than half the required time to bill for them (e.g., eight minutes for a 15-minute service). This is known as the midpoint rule.3 If the code description instead includes a time range (e.g., 5–15 minutes), physicians only need to spend the minimum time listed to bill for the service. Make sure to document how many minutes you spent if time is a required component for billing. Below are some examples common to family medicine.
Tobacco cessation counseling: Tobacco cessation counseling is a covered service for anyone who uses tobacco. Medicare Part B covers up to eight tobacco counseling visits each year, using CPT codes 99406 (0.24 RVUs) and 99407 (0.50 RVUs) paired with an ICD-10 code that describes the patient’s tobacco use (see “Diagnosis codes associated with counseling and screening services”).
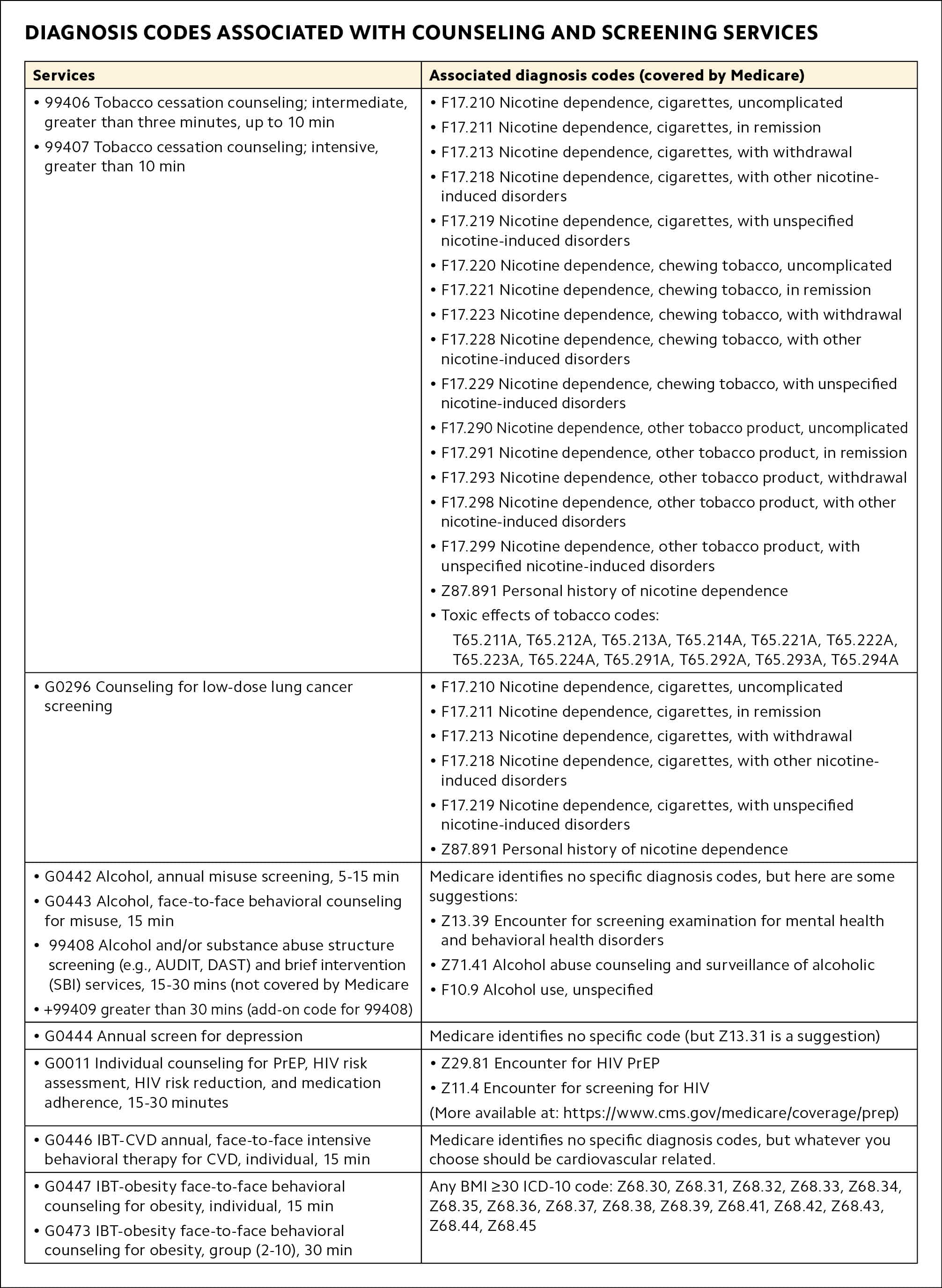
| Services | Associated diagnosis codes (covered by Medicare) |
|---|---|
|
|
|
|
| Medicare identifies no specific diagnosis codes, but here are some suggestions:
|
| Medicare identifies no specific code (but Z13.31 is a suggestion) |
|
|
| Medicare identifies no specific diagnosis codes, but whatever you choose should be cardiovascular related. |
| Any BMI ≥30 ICD-10 code: Z68.30, Z68.31, Z68.32, Z68.33, Z68.34, Z68.35, Z68.36, Z68.37, Z68.38, Z68.39, Z68.41, Z68.42, Z68.43, Z68.44, Z68.45 |
Low-dose CT scan lung cancer screening counseling: Asymptomatic patients ages 50–80 who have at least a 20-pack-year smoking history and either currently smoke or have quit within the past 15 years may be eligible for low-dose lung cancer screening (CPT 71271) and pre-screening counseling (G0296; 0.52 RVUs). Traditional Medicare covers this only up to age 77, but other payers may follow the U.S. Preventive Services Task Force guidelines, which recommend screening up to age 80. The screening itself requires a computed tomography (CT) scan, which is a separate procedure code, but primary care physicians may bill for counseling patients about the screening — including eligibility — and shared decision making.
Alcohol misuse screening and counseling: Medicare covers alcohol misuse screening once a year, and if the patient screens positive, it covers four additional face-to-face counseling sessions per 12-month period. The codes are G0442 (15-minute annual alcohol misuse screening, 0.18 RVUs) and G0443 (15-minute face-to-face behavioral counseling for alcohol misuse, 0.60 RVUs). Non-Medicare plans may use 99408 (15–30 minute structured alcohol or substance abuse screening and brief intervention, 0.65 RVUs) and +99409 (add-on code for 99408 longer than 30 minutes, 1.30 RVUs).
Depression screening: Medicare covers an annual depression screening with code G0444 (0.18 RVUs) as a billable service when staff-assisted depression care supports are in place to ensure accurate diagnosis, effective treatment, and follow-up care, helping to facilitate and coordinate mental health referrals. No specific screening tool is required, but you should document what tool you used. There is a 5-15 minute time requirement for this service.
Pre-exposure prophylaxis (PrEP) counseling and screening: Medicare covers 15–30 minutes of HIV PrEP counseling with G0011 (0.45 RVUs) as a preventive service for individuals at increased risk of HIV acquisition (most other payers do as well).4 It also covers up to eight counseling sessions and up to eight screening tests every 12 months. The counseling sessions include risk assessment, risk reduction, and medication adherence.
Intensive behavioral therapy (IBT) for cardiovascular disease risk: Clinicians use IBT codes for risk-reduction counseling. When used for cardiovascular disease (CVD) risk reduction, the service includes three main components: 1) encouraging aspirin use for the primary prevention of CVD when the benefits outweigh the risks for men age 45–79 years and women age 55–79 years, 2) screening for high blood pressure, and 3) intensive lifestyle counseling to prevent CVD. The code is G0446 (0.60 RVUs). Bill this service with the diagnosis code for the condition that puts the patient at high risk for CVD. It can be billed once a year.
IBT for obesity: Use G0447 (0.60 RVUs) to report IBT for obesity for an individual patient (15 minutes) and G0473 (0.23 RVUs) for a group of 2–10 patients (30 minutes). They must be associated with a diagnosis code showing the patient’s BMI is 30 or above, and must include a nutritional assessment and intensive lifestyle counseling to promote sustained weight loss through high-intensity interventions focused on diet and exercise. This can be billed up to 22 times per 12-month period, with the following frequency:
- First month: one face-to-face visit every week,
- Months 2–6: one face-to-face visit every other week,
- Months 7–12: one face-to-face visit every month, if patient loses at least three kilograms (6.6 pounds) during the first six months.
GENERAL PREVENTIVE COUNSELING SERVICES
Most primary care physicians are familiar with preventive medicine E/M codes (e.g., 99381-99387 and 99391-99397) for well-child visits, annual exams, or preventive visits. But other preventive medicine counseling codes can be billed for general risk-factor reduction, promoting health, and preventing illness. Because these are general counseling services, you can use diagnosis codes Z00.00 (general adult medical exam without abnormal findings) or Z00.01 (general adult medical exam with abnormal findings). If you discuss more specific issues, you could use codes such as Z71.3, “Dietary counseling and surveillance” and Z71.82, “Exercise counseling.” If these are services that you will routinely provide, it is best practice to reach out to the payer to see if they require specific diagnosis codes.
Preventive medicine counseling and/or risk factor reduction: The CPT codes below would be reimbursed by commercial payers, Medicaid, and some Medicare Advantage plans:
- 99401 15 min (0.48 RVUs),
- 99402 30 min (0.98 RVUs),
- 99403 45 min (1.46 RVUs),
- 99404 60 min (1.95 RVUs),
- 99411 group setting; 30 min (0.15 RVUs),
- 99412 group setting; 60 min (0.25 RVUs).
Prolonged preventive services: These G codes — G0513 and G0514 — are reimbursed by Medicare for preventive services that extend beyond the typical service time of the primary procedure, are provided in the office or other outpatient setting, and require direct patient contact beyond the usual service. Use G0513 for the first 30 minutes (1.17 RVUs) and G0514 for each additional 30 minutes (1.17 RVUs). These should be billed on a very rare basis.
WOMEN’S HEALTH SCREENING SERVICES
The following women’s health screenings are separately billable services for Medicare, but not for commercial payers or Medicaid (where they are bundled into well-woman visits).
Pelvic/breast exam: To bill G0101 (0.45 RVUs), you must examine at least seven of 11 areas. One of them must be a breast exam that includes inspection and palpation of the breasts. A digital rectal exam is optional. The rest of the seven come from a pelvic exam that can include any of the following areas (with or without specimen collection for smears and cultures):
- External genitalia,
- Urethral meatus,
- Urethra,
- Bladder,
- Vagina,
- Cervix,
- Uterus,
- Adnexa/parametria,
- Anus and perineum.
Document in the note which areas you examined. Find more details on the Centers for Medicare & Medicaid Services coverage determination page.5
Pap smear: Use HCPCS code Q0091 (0.37 RVUs) for Medicare patients who still need a Pap smear, even if you provided this service in addition to a wellness visit.
You may bill Medicare for G0101 and Q0091 annually (or 11 months after the month of the previous covered exam) for women at high risk for developing cervical or vaginal cancer, or women of childbearing age with an abnormal Pap test within the past 36 months. Otherwise, they’re billable once every 24 months (or 23 months after the month of the previous covered exam) for low-risk women. Make sure your diagnosis code indicates high risk or low risk. Most women on Medicare are outside the recommended age range (21–64) for these screenings, but there are younger women on Medicare due to disability or other qualifying diseases who require these services.
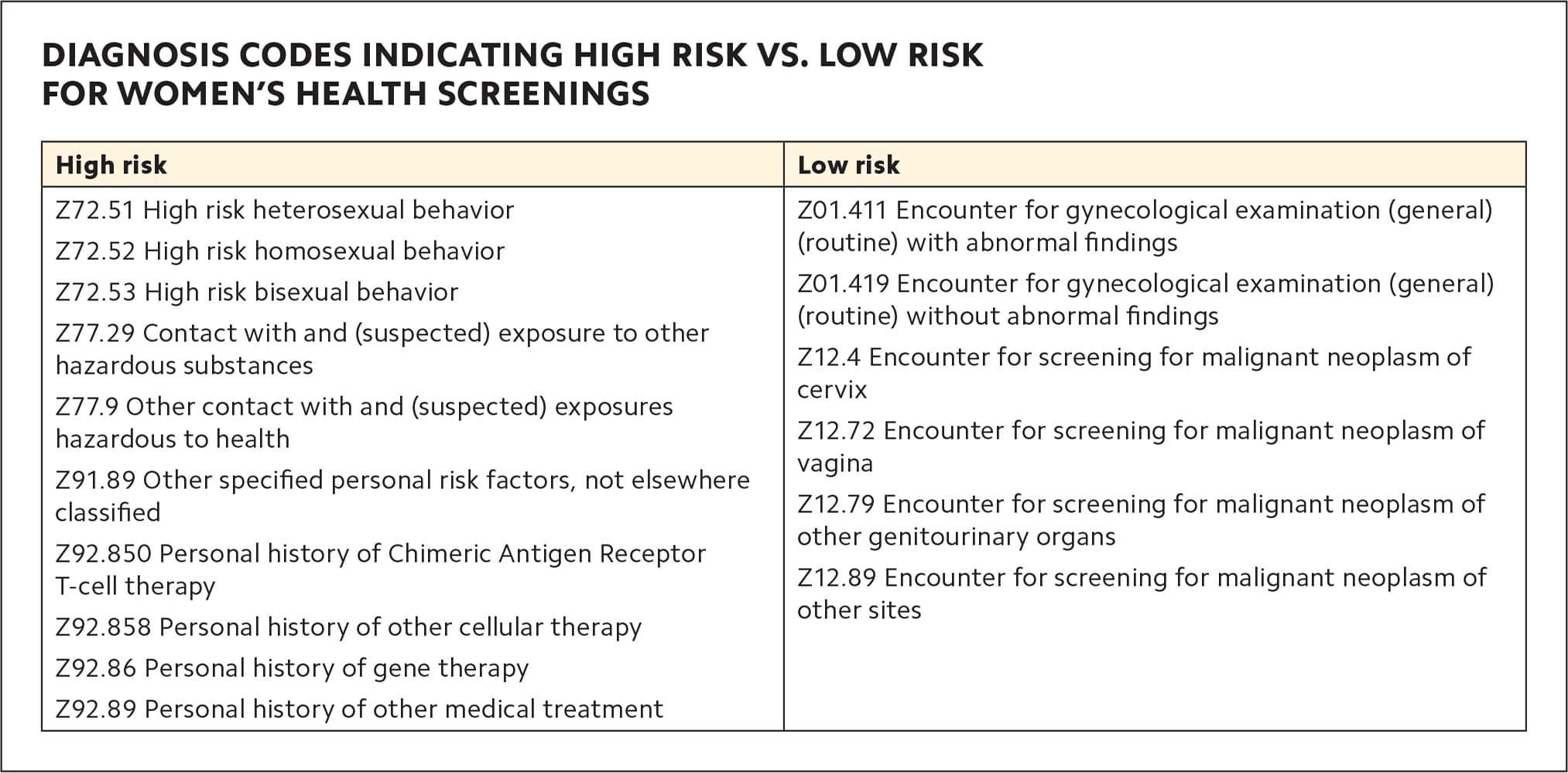
| High risk | Low risk |
|---|---|
| Z72.51 High risk heterosexual behavior Z72.52 High risk homosexual behavior Z72.53 High risk bisexual behavior Z77.29 Contact with and (suspected) exposure to other hazardous substances Z77.9 Other contact with and (suspected) exposures hazardous to health Z91.89 Other specified personal risk factors, not elsewhere classified Z92.850 Personal history of Chimeric Antigen Receptor T-cell therapy Z92.858 Personal history of other cellular therapy Z92.86 Personal history of gene therapy Z92.89 Personal history of other medical treatment | Z01.411 Encounter for gynecological examination (general) (routine) with abnormal findings Z01.419 Encounter for gynecological examination (general) (routine) without abnormal findings Z12.4 Encounter for screening for malignant neoplasm of cervix Z12.72 Encounter for screening for malignant neoplasm of vagina Z12.79 Encounter for screening for malignant neoplasm of other genitourinary organs Z12.89 Encounter for screening for malignant neoplasm of other sites |
MISCELLANEOUS SERVICES
Other services primary care physicians routinely provide but do not code are listed below. Two that can be added to a Medicare annual wellness visit (AWV) without a co-pay are social determinants of health (SDOH) risk assessment and advance care planning.6,7 In both cases, add modifier 33 to the code to waive cost sharing for the patient when billing with a Medicare AWV. (You can also bill SDOH risk assessment and advance care planning separately with an E/M visit, but a co-pay would apply.)
SDOH risk assessment: The SDOH risk assessment (G0136, 0.18 RVUs) should take 5–15 minutes and can be reported every six months. It is not intended to be a routine screening but is administered when the physician believes there is an unmet need that may impact diagnosis and treatment. No specific screening tool is required, but it must be standardized and evidence based. Use ICD-10 “Z” codes when applicable.8 If none of the existing Z codes are relevant, use your own discretion about which diagnosis code fits.
Advance care planning: This is a voluntary, face-to-face discussion with the patient about their health care wishes should they become unable to make their own medical decisions. It can include talking about advance directives, with or without helping a patient complete legal documents. No specific ICD-10 code is required to bill this service, and there is no limit on how frequently you can report it. However, billing it more than once can be a red flag for audits, and Medicare will expect to see that the patient’s status or wishes have changed. Use 99497 (1.50 RVUs) for the first 30 minutes and 99498 (1.40 RVUs) for every additional 30 minutes.
Home health certification: Completing paperwork to certify patients for home health is a billable service for Medicare. The patient does not have to be present, but the physician must have had a previous face-to-face encounter with the patient and must be the one supervising the care of the patient. There is no time component for billing this service. The initial service (G0180, 0.67 RVUs) is billable once per certification period when the patient has not received home health services for at least 60 days. Bill for recertification using G0179 (0.45 RVUs) every 60 days after the initial 60 days, within a five-day window before the start of the next period (Medicare will deny it any time prior to that). Add a place of service code where the majority of the planning occurred. Your documentation must show contact with the home health agency and review of patient status reports.
Care plan oversight: Physicians can also bill for monthly care plan oversight for patients in home health or hospice who require complex or multidisciplinary care. These services include regular development or revision of care plans (including integration of new information in the treatment plan and medication adjustments); review of patient status reports, labs, and other studies; and communication (including telephone calls) with the patient’s other health care professionals, family members, or caregivers.
The home health oversight codes are G0181 for Medicare and CPT 99375 for commercial payers. The hospice care oversight codes are G0182 for Medicare and 99378 for commercial payers (all are 1.73 RVUs). All require at least 30 minutes per month (CPT includes other codes for less than 30 minutes, but commercial payers often do not reimburse for them because they follow Medicare rules). Track your time each month and include it in your documentation.
Transitional care management: Primary care physicians are routinely scheduled to see patients after discharge from a hospital, inpatient rehab facility, or skilled nursing facility — even if it’s not their patient. These visits, known as transitional care management (TCM), usually require more review and medical decision making than typical E/M visits and reimburse at a higher level. However, they also require communication with the patient or caregivers within two business days of discharge. The communication must be performed by either the physician or clinical staff under the direction of the physician, and it can be done by phone, by email, or face-to-face.9 If you make two or more unsuccessful attempts to contact the patient during that period but eventually are able to see the patient for the visit, you may still bill the service, but make sure to document your attempts. TCM also includes medication reconciliation and management, as well as communicating with social service agencies the patient uses and identifying other community resources that might be available (staff may do this under your supervision).
The CPT codes for TCM are 99495 (2.78 RVUs) for moderate-complexity medical decision making (requires face-to-face visit within 14 calendar days of discharge) and 99496 (3.79 RVUs) for high-complexity medical decision making (requires face-to-face visit within seven days of discharge).
PUTTING IT INTO PRACTICE
The RVUs tied to these services may seem small, but if you find yourself spending a lot of time counseling patients or providing services in addition to chronic disease management, they can add up quickly. Counseling is a key part of primary care, and physicians should be paid for the services they are performing.
To show how this works in practice, let’s consider a hypothetical patient, Michael. He’s a 67-year-old who comes in for a medication refill and follow-up care for knee pain. Your medical assistant completed a PHQ-9 depression questionnaire during the rooming process and told you Michael’s score was eight. You check his blood pressure, adjust his medication dosage, and send in a prescription with a new dose. You also examine his knee, review his previous X-ray, and send a referral to physical therapy. This would typically be billed as 99214 with 1.92 RVUs.
However, you start talking to Michael about his PHQ-9 results and ask why he has been feeling down and having trouble sleeping. This leads you to talk about his tobacco use, provide tobacco cessation counseling, and screen for alcohol use. You recognize Michael has been using alcohol to deal with family issues. This leads you to provide counseling for alcohol misuse, additional resources, and a referral. You talk to Michael about counseling and medication for his mild depression and ask him to schedule a follow-up visit in two weeks.
In the end, this seemingly simple chronic disease management visit required additional services. Instead of just billing a 99214 for managing the chronic conditions, you can also bill for depression screening (G0444, 0.18 RVU), tobacco cessation counseling (99406, 0.24 RVU), alcohol misuse screening (G0442, 0.18 RVU), and alcohol misuse counseling (G0443, 0.60 RVU), for a total of 3.12 RVUs. Plus, the additional counseling will help with risk-factor modification and hopefully help him better manage the chronic conditions he came in for.
So don’t forget to document all the services you are providing to keep your patients healthy and out of the hospital, as these are billable services that benefit the patient and account for the time you spent.
