
Regular access to primary care is key to health and well-being, even for physicians.

In 2022, the U.S. surgeon general issued an advisory defining physician burnout as an urgent public health issue.1 The advisory recommended prioritizing care-seeking strategies and basic health habits for physicians. One such habit is regularly following up with a primary care physician.
Physicians face both individual and systemic barriers to seeking primary care. This article examines the literature on physicians’ access to primary care physicians, identifies common barriers, and offers potential solutions.
KEY POINTS
- Prioritizing care-seeking strategies and basic health habits is a key part of reducing burnout, and it includes physicians receiving regular care from a primary care physician.
- Physicians face systemic barriers to seeking primary care, including lack of time and concerns about confidentiality.
- Starting during training, physicians should be encouraged to practice self-care behaviors, should establish care with a primary care physician, and should be taught how to support their medical colleagues as patients.
WHY PHYSICIANS NEED THEIR OWN PHYSICIAN
Regular access to a primary care physician can improve physician wellness by ensuring that any physical and mental health issues are being addressed in a timely fashion. Currently, more than 300 physicians die by suicide each year, and many more suffer from depression and anxiety.2 The COVID-19 pandemic led to an increase in mental health and substance use visits among physicians, contributing to an increased need for access to mental health services.3 Yet, among physicians who identified as having depression, only 25% considered getting help and only 2% received it.4
Integrating mental health into primary care can have significant benefits.5 A Department of Veterans Affairs study showed that integration led to decreased rates of mental health specialty use.6 At a time when there is a high prevalence of mental health diagnoses and a shortage of mental health providers, integration improves access to mental health care.7 In addition, chronic work-related stress makes physicians more vulnerable to certain physical conditions, such as impaired cognitive function, heart disease, and type 2 diabetes.1 However, physicians frequently minimize or downplay their experience of stress.7 Without a primary care physician, physicians as patients risk trivializing their symptoms, over-treating in some cases, and self-treating without proper documentation, leading to gaps in care.8
LITERATURE ON PRIMARY CARE USAGE BY PHYSICIANS
Years ago, a cohort study of physicians who graduated from Johns Hopkins School of Medicine found that not having a regular source of care predicted gaps in recommended screenings for breast, colon, and prostate cancer as well as seasonal influenza vaccines.9 More recent studies on the topic of primary care usage by physicians are mostly from other countries and include the following findings:
- Compared to nonphysicians, doctors were less likely to be enrolled with a primary care physician10 and had lower rates of periodic health exams and screenings for hyperlipidemia and diabetes,11
- Physicians were less likely than the general population to follow health maintenance guidelines,12
- Half of doctors did not have an established relationship with a primary care clinician, nearly 90% believed it was acceptable to self-treat acute conditions, and 9% indicated it was appropriate to self-prescribe psychiatric medications,13
- Nearly a third of physicians had not seen a primary care physician in the last five years, and about 92% of them had self-prescribed medications at least once,14
- Physicians exhibited behaviors such as self-diagnosing conditions, minimizing their symptoms, neglecting their health, and engaging in “corridor consultations,”15,16 informal conversations with colleagues about their health issues.
Unlike the U.S. health care system, the National Health Service requires residents of the United Kingdom (including physicians) to register with a “general practitioner.” Studies have found that doctors who regularly see a personal physician are more likely to receive preventive services.17 Similarly, one study revealed that surgeons who saw their primary care physician in the prior year were more likely to engage in aerobic exercise and participate in wellness programs, and they had higher quality-of-life scores.18 In another study, surgeons who had seen their primary care physician in the last 12 months were more likely to be up to date on health screenings.2
BARRIERS TO PHYSICIANS SEEKING CARE
Physicians encounter both systemic and individual roadblocks to seeking care.
The top two systemic barriers are lack of time and concerns about confidentiality.15 Often, their professional commitments interfere with seeking medical care because it is difficult to schedule an appointment during work hours, especially without a backup.19–22 Doctors are also concerned about their confidentiality, especially those who practice in rural/geographically isolated areas.23 Professional licensure barriers further dissuade physicians from seeking care related to mental health.21,22 Some licensing boards ask questions about applicants’ history of physical health, mental health, and substance abuse even if these conditions are not active nor directly impacting patient care.4
Individual factors also serve as roadblocks. Doctors often carry a perception that they don’t get sick.22 The traits of perfectionism combined with the medical culture of self-sacrifice discourage physicians from taking care of their own health.4 In one study, primary care physicians indicated that the need to portray a healthy image hindered them from acknowledging personal illnesses and engaging in preventive screenings.24 Doctors also exhibit “post-residency disease,” when they downplay their physical symptoms and delay seeking care, thus earning the title of “bad patients.”21,25
STRATEGIES TO IMPROVE PRIMARY CARE DELIVERY TO PHYSICIANS
While there is limited evidence on successful interventions to improve access to primary care for physicians, we offer several strategies in two key areas:
1. Encourage self-care behaviors, starting during medical training. Medical students are rarely taught how to approach their own health concerns.26 Prior to starting medical school, students exhibit “anticipatory socialization,” a process of adopting new skills and behaviors to prepare for their roles as future physicians.25 As they go through training, their professional “doctor” identity and personal identity become intertwined, and they learn that being a “doctor” is synonymous with not being a patient.25 For this reason, it is most effective to begin self-care training during medical school.27 Medical students and resident physicians should be encouraged to have a primary care physician and follow up on a regular basis. One study found that healthy behaviors present in medical school declined during residency.28 Thus, developing connections to primary care physicians during medical school could reduce barriers to sustaining healthy lifestyle efforts thereafter.
2. Encourage physicians to establish care with a primary care physician, especially during the onboarding process for new hires. To enable this, practices could designate time slots on the work schedule for these appointments. Arranging adequate backup could also encourage physicians to see their own physicians when they are sick.19 To improve accessibility, telehealth and virtual care options could be considered.1 These may be especially helpful for physicians in rural settings. Since privacy is a concern to seeking care, additional EHR confidentiality and security measures should be offered, such as “break-the-glass” tools, which prompt users who do not have a known relationship with a patient to select the specific purpose before accessing the chart. Physicians must also be allowed to seek care at other institutions if they choose.
3. Improve interactions between physician-patients and their primary care physicians. For primary care physicians, taking care of physician-patients comes with its own set of challenges: maintaining boundaries, making assumptions about the physician-patient’s medical knowledge and health behaviors, and maintaining the physician-patients’ access to personal test results and informal consultations.29 In addition, physicians may feel hesitant to perform a more comprehensive physical exam on physician-patients and may do a less rigorous follow-up, assuming the physician-patient will contact them if they develop concerning symptoms.27,30 In a recent study, primary care physicians reported having increased stress while seeing physician-patients, and 52% reported that their physician-patients tried to control their own care.31 Some primary care physicians were willing to be more lenient with scheduling and testing for physician-patients, but as their experience increased, primary care physicians felt more comfortable following a protocol and maintaining boundaries.31
Primary care physicians should be provided training on how to support their medical colleagues as they become patients. To improve these interactions, both parties must be clear about their roles. The primary care physician should ask about the physician-patient’s self-diagnosis and address their concerns about privacy and confidentiality. And they should discuss diagnostic and treatment plans in detail without making any assumptions about prior knowledge and leave adequate time for discussion of the plan.30,32
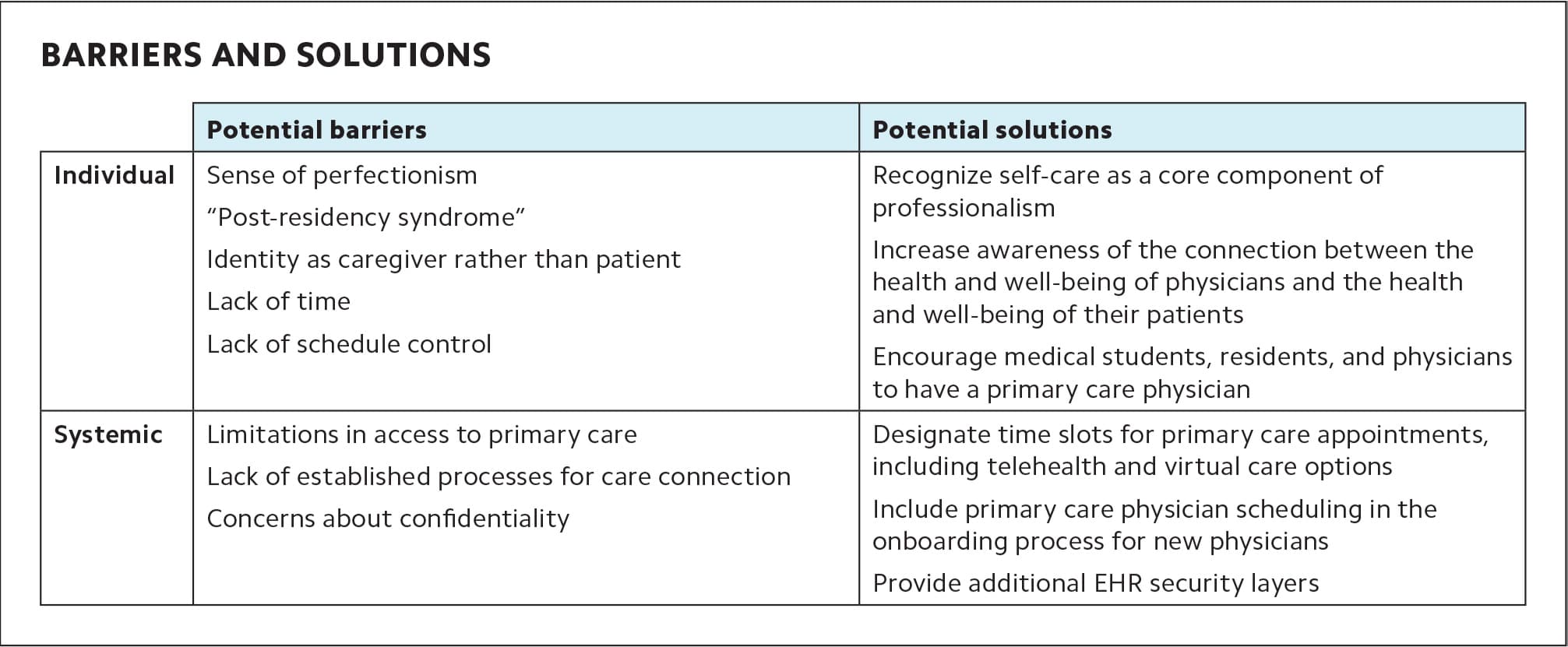
BARRIERS AND SOLUTIONS
| Potential barriers | Potential solutions | |
|---|---|---|
| Individual | Sense of perfectionism “Post-residency syndrome” Identity as caregiver rather than patient Lack of time Lack of schedule control |
Recognize self-care as a core component of professionalism Increase awareness of the connection between the health and well-being of physicians and the health and well-being of their patients Encourage medical students, residents, and physicians to have a primary care physician |
| Systemic | Limitations in access to primary care Lack of established processes for care connection Concerns about confidentiality |
Designate time slots for primary care appointments, including telehealth and virtual care options Include primary care physician scheduling in the onboarding process for new physicians Provide additional EHR security layers |
PUTTING IT INTO PRACTICE
Regular access to primary care is the vital first step to promoting wellness, even among physicians. While lack of time, confidentiality concerns, and the prevailing culture of perfectionism block physicians from seeking primary care, systemic changes can help dismantle these roadblocks. The solutions described above may sound obvious, but putting them into practice will require a collaborative effort from health systems, medical training institutions, and physicians. Because the problem of physician burnout is multifactorial, a more holistic approach is needed to promote physician wellness.
