Acid-Base and Electrolyte Disorders
Sections One and Two of this monograph review electrolyte disorders of sodium and potassium, the importance of normal electrolyte levels for cellular function, and the clinical manifestations of and evaluations and treatments for abnormalities. Section Three explores acid-base disorders, with a focus on how family physicians can correctly interpret laboratory values. Section Four reviews the clinical presentation, diagnosis, and treatment of hypocalcemia and hypercalcemia.
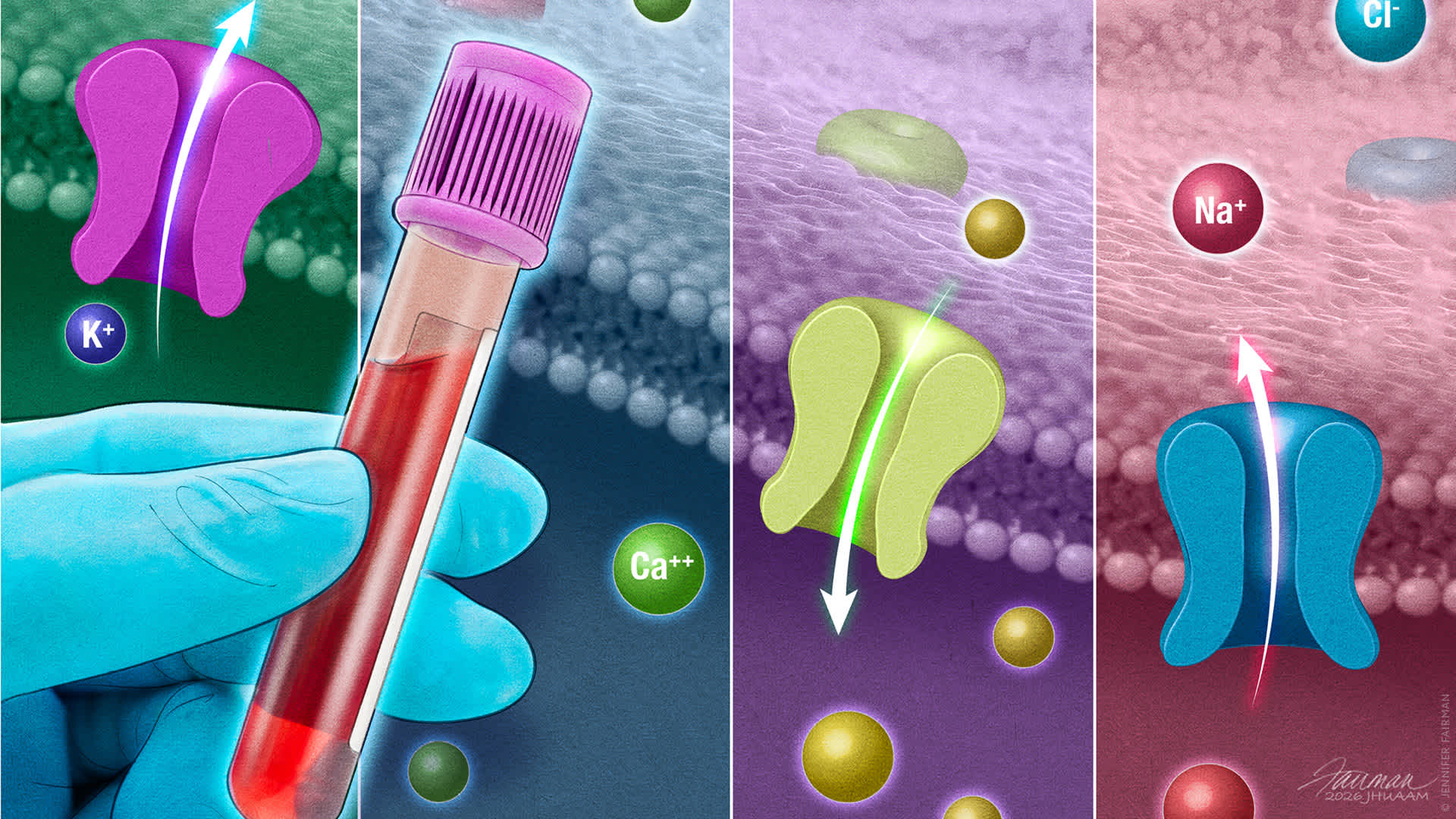
Potassium Disorders
A normal serum potassium level of 3.5 to 5.0 mEq/L is maintained via potassium ingestion, excretion, and distribution between intra- and extracellular fluid. Potassium balance is essential for maintenance of normal resting cell membrane potential in excitatory tissues. Abnormalities in serum potassium, whether low or high, can cause life-threatening complications due to cardiac, respiratory, or neurologic compromise. Hypokalemia results from renal or gastrointestinal losses, or transcellular shifts. In the absence of an identified cause, evaluation of urinary potassium excretion and acid-base status can help determine the etiology. Patients with severe (ie, serum potassium less than 2.5 mEq/L) or symptomatic hypokalemia should be admitted to the hospital for intravenous potassium replacement and cardiac monitoring. Patients with mild to moderate hypokalemia are often asymptomatic and can be treated with oral potassium while the underlying cause is addressed. Hyperkalemia is usually due to low urinary excretion, and less often to cellular release and transcellular shifts. Patients with acute hyperkalemia with associated electrocardiography findings and those with potassium levels 6.5 mEq/L or greater require inpatient treatment with calcium gluconate and other measures. Asymptomatic patients with chronic mild to moderate hyperkalemia can be managed as outpatients with dietary modification, diuretics, and medication adjustments.
Acid-Base Disorders
Maintaining a normal physiologic acid-base balance is essential for the functioning of every organ system in the body. The renal and pulmonary systems are the primary regulators of acid-base balance. There are four principal acid-base disorders: metabolic acidosis, metabolic alkalosis, respiratory acidosis, and respiratory alkalosis. A systematic approach to evaluation is critical to identify potential etiologies. A history, physical examination, metabolic profile, and arterial blood gas measurement provide a full assessment of acid-base status. However, availability of arterial blood gas measurements is usually limited outside of inpatient and emergency department settings. Calculation of an anion gap is a crucial first step for evaluating laboratory test results. Changes in serum pH, Pco2, serum bicarbonate concentration, and anion gap suggest the primary disorder, and predictable compensatory changes indicate whether a secondary acid-base disturbance is present. Mixed acid-base disorders involving the renal and pulmonary systems can occur, underscoring the importance of a systematic approach to evaluation. In the outpatient setting, primary care physicians play a vital role in identifying and treating these disorders based on initial evaluation. Prompt recognition and management of acid-base disorders can help prevent morbidity and mortality.
Calcium Disorders
Calcium is an essential element for normal physiologic function. Normal serum calcium is maintained within a close range of 8.4 to 10.4 mg/dL, and acute or severe changes can result in serious cardiac, musculoskeletal, and neurologic consequences. Normal calcium levels are maintained by interactions of parathyroid hormone and vitamin D. Parathyroid hormone regulates calcium levels via bone resorption, renal calcium reabsorption, and enhanced calcium absorption in the small intestine. Causes of hypocalcemia include hypoparathyroidism (often postsurgical), severe chronic kidney disease, and vitamin D deficiency. Laboratory testing for serum parathyroid hormone, kidney function, vitamin D metabolites, and serum phosphorus can help differentiate among causes. Acutely symptomatic patients require inpatient treatment with intravenous calcium gluconate, cardiac monitoring, and correction of hypomagnesemia. Hypercalcemia is most often due to primary hyperparathyroidism or malignancy. In the evaluation, hypercalcemia should first be confirmed by measurement of ionized calcium or repeat measurement of total serum calcium and correction for albumin. Obtaining a serum parathyroid hormone level is the next step. Asymptomatic, chronic mild hypercalcemia is often caused by primary hyperparathyroidism, which can be observed or treated surgically. Patients with severe hypercalcemia may have profound dehydration and require inpatient treatment with intravenous fluids, bisphosphonates, and calcitonin.
Past Editions
#564 | Skin Cancer
See full issue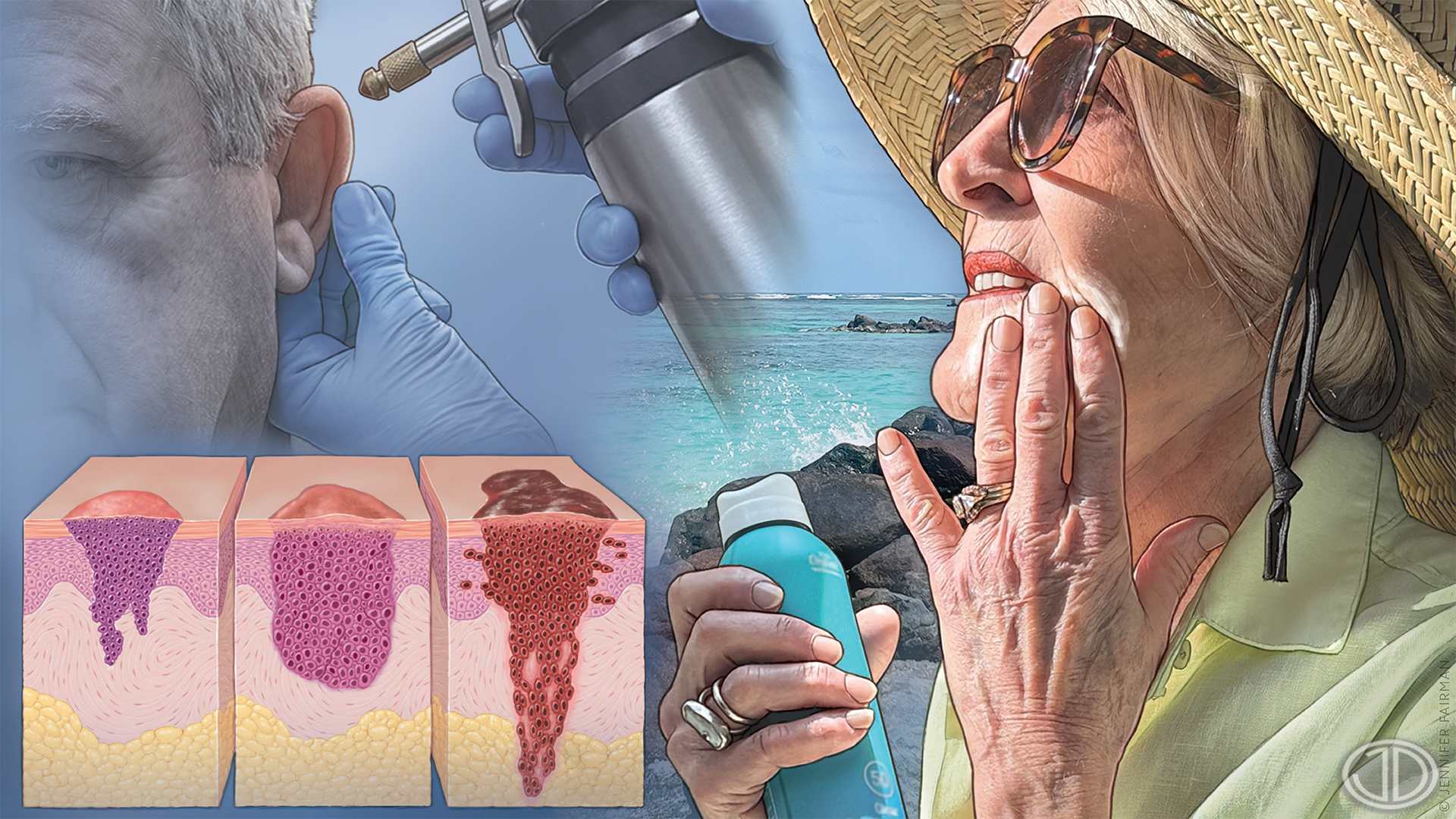
Screening and Prevention
Skin cancer is the most common cancer in the United States. Basal cell carcinoma, the leading type of skin cancer across all racial and ethnic groups, is usually slow growing and curable. Cutaneous squamous cell carcinoma accounts for more skin cancers in individuals with…
Diagnosis
Family physicians play a critical role in early detection of skin cancers. Although visual inspection is the initial step, dermoscopy significantly improves diagnostic accuracy, particularly for melanoma and basal cell carcinoma. Advanced imaging technologies such as…
Management of Actinic Keratoses and Keratinocyte Carcinomas
Actinic keratoses are precancerous skin lesions that are treated to prevent progression to cutaneous squamous cell carcinoma. Keratinocyte carcinomas include basal cell carcinoma and cutaneous squamous cell carcinoma. Cryosurgery is preferred to treat a single or limited number…
Management of Cutaneous Melanoma
Melanoma is the fifth most common cancer in the United States and one of the deadliest. Tumor depth (Breslow depth) is the most important prognostic factor. Wide local excision is used to manage melanoma stage 0 (in situ) with 0.5- to 1-cm margins, as well as stage IA with 1-cm…