
Alcohol use during pregnancy increases health risks for the developing baby, ranging from miscarriage and sudden infant death syndrome to preterm birth and developmental problems.1 Fetal alcohol spectrum disorders (FASDs) encompass a series of diagnostic categories that may occur due to alcohol exposure during pregnancy.2 When alcohol crosses the placenta, the result is damaged fetal cells, which inhibit nutrient uptake and impact organ systems and fetal development.3 Secondary and cooccurring conditions are common among people with FASDs and include a broad range of physical and mental health diagnoses.4
Epidemiology
The true prevalence of alcohol-exposed pregnancies is not known. However, self-reported alcohol use findings from the National Survey on Drug Use and Health and the Behavioral Risk Factor Surveillance System include5,6:
- Alcohol use in the past month among all reproductive age females 15–44 years was 47.4% in 2024.
- Eight percent of women 18 years and older had a past-year alcohol use disorder in 2024.
- Nearly 1 in 20 (4.7%) of pregnant respondents reported past-month alcohol use in 2024 (8.4% in 2023).
- Pregnant binge drinking (four or more standard drinks in two hours) rates were also down from 4.8% in 2023 to 1.2% in 2024.
These recent data are encouraging, as there has been some decreases in alcohol use among these populations. However, significant risks for alcohol-exposed pregnancy persist, as overall alcohol use is still high in reproductive age females, as is the rate of unplanned pregnancies, which can result in unintended alcohol exposure in early pregnancy.
Prevalence of FASDs has been estimated to be as high as 1% to 5% of U.S. school children, but more research is needed.7 FASDs are underdiagnosed, as screening, diagnosis and treatment are not universally available or uniform, and many co-occurring conditions complicate the identification of FASDs.8 Furthermore, estimates vary regarding rates of undiagnosed FASDs present in the criminal justice system, but experts suggest significant overrepresentation and underdiagnosis.9
Signs, Symptoms, Secondary and Co-occurring Conditions and FASDs
Neurodevelopmental: Microcephaly, brain abnormalities, spinal cord malformations, developmental delay, intellectual disability, executive dysfunction, learning disabilities, language disorders, autism spectrum disorder-like features, seizures, impaired social cognition, stress-axis dysregulation
Growth: Low birth weight, prenatal and postnatal growth restriction, failure to thrive
Craniofacial/orofacial: Characteristic facial dysmorphology (e.g., smooth philtrum, short palpebral fissures, midfacial hypoplasia), cleft lip and/or palate, dental and orthodontic abnormalities
Vision/ophthalmologic: Ptosis, strabismus, retinal malformations, structural eye abnormalities, visual impairment
Auditory/otologic: Chronic otitis media, hearing loss, microtia, structural ear deformities
Cardiac: Heart defects, atrial septal defect, ventricular septal defect, aberrant great vessels
Renal/genitourinary: Renal agenesis, renal dysplasia, renal hypoplasia, renal fusion, hydronephrosis, ureteral duplication
Musculoskeletal: Camptodactyly, clinodactyly, flexion contractures, hypoplastic nails, radioulnar synostosis, scoliosis, vertebral malformations
Behavioral/mental health: Behavioral dysregulation, emotional regulation difficulties, conduct disorder, ADHD, oppositional defiant disorder, substance use disorder (adolescence and adulthood)
Prevention
Alcohol use during pregnancy is the sole cause of FASDs. Therefore, it is preventable with adequate awareness for people at risk. There is no known safe amount, no safe time and no safe type of alcohol use during pregnancy. The only way to prevent FASDs is to avoid all alcohol during pregnancy, including before a woman knows she is pregnant, which includes while planning to become pregnant or at risk of pregnancy. If a fetus is exposed to alcohol before pregnancy recognition, then discontinuing alcohol consumption as soon as a pregnancy is known is the best way to reduce the potential impact.
Public health education campaigns and health professional training are key to raising awareness. Alcohol use interventions in primary care, such as Screening, Brief Intervention, and Referral to Treatment (SBIRT), help to educate patients and intervene to reduce alcohol and substance use before, during and after pregnancy.12 The U.S. Preventive Services Task Force recommends screening for unhealthy alcohol use among adults, including pregnant women.13 More alcohol and substance use treatment availability is needed to meet demand and support the prevention of FASDs. Tertiary prevention interventions for children and families living with FASDs—such as family therapy, mentoring and caregiver support groups—also have beneficial impacts, preventing unnecessary negative experiences and outcomes.14
Screening and Diagnosis
Screening for FASDs should be considered for anyone with known prenatal alcohol exposure or identified growth retardation, facial dysmorphology, central nervous system (CNS) dysfunction or neurobehavioral disabilities.15 While there is no single diagnostic test for FASDs, several diagnostic approaches are available. There is also no definitive “best” approach, as each entails trade-offs between sensitivity and specificity due to challenges in defining developmental and exposure criteria, setting thresholds and classifying FASDs.
Sentinel Facial Features of a Child with FASDs
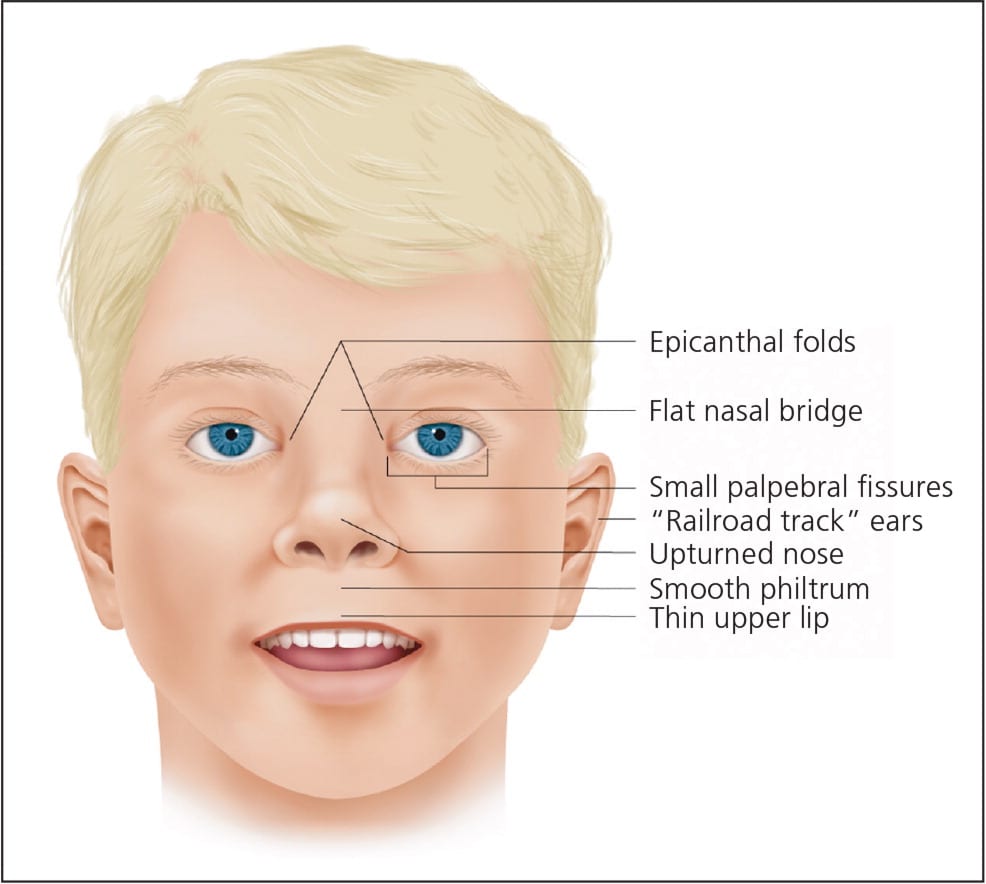
Reprinted with permission from Wattendorf D, Muenke M. Fetal alcohol spectrum disorders. Am Fam Physician. 2005;72(2):279–285.
One of the two most used diagnostic systems in the United States is the Collaboration on FASD Prevalence criteria, which uses the following broad but sensitive categories16–18:
Fetal alcohol syndrome is a combination of diagnostic indicators, including characteristic facial features, growth problems, CNS effects, and cognitive and behavioral challenges with learning, memory, attention, communication, vision, hearing, and academic and social difficulty.
Partial fetal alcohol syndrome is a more limited set of diagnostic indicators, including a combination of a known history of prenatal alcohol exposure, some characteristic facial features and a growth problem or CNS effects.
Alcohol-related neurodevelopmental disorder criteria include intellectual disabilities and problems with behavior and learning.
Alcohol-related birth defects include a range of problems with the heart, kidneys, bones, vision and hearing.
Neurobehavioral disorder associated with prenatal alcohol exposure diagnostic criteria include known alcohol exposure, challenges with thinking and memory, behavior and mood issues, and other developmental and social effects. This diagnosis was added to the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition, Section III conditions for further study in 2013.
Alternatively, the University of Washington 4-Digit Diagnostic Code is a more specific diagnostic system that uses ordinal rankings to classify a continuous range of diagnoses and severities.19 Both systems agree on the importance of using a multidisciplinary approach to evaluate prenatal alcohol exposure, facial and other dysmorphology, and developmental and behavioral indicators.8,16
The multidisciplinary team and neuropsychological assessment can include a wide range of specialists as appropriate, such as a family physician or pediatrician, geneticist, psychologist or psychiatrist, neurologist, social worker, early intervention services, educational specialist, family therapist, physical therapist, and speech pathologist.20 Diagnostic challenges are compounded by the array of other possible contributors to fetal and childhood developmental problems, necessitating a thorough and multidisciplinary differential diagnosis. Confounders can include other developmental delays, multiple teratogen exposures, adverse childhood experiences and genetic syndromes.8
Example of the 4-Digit Diagnostic Code
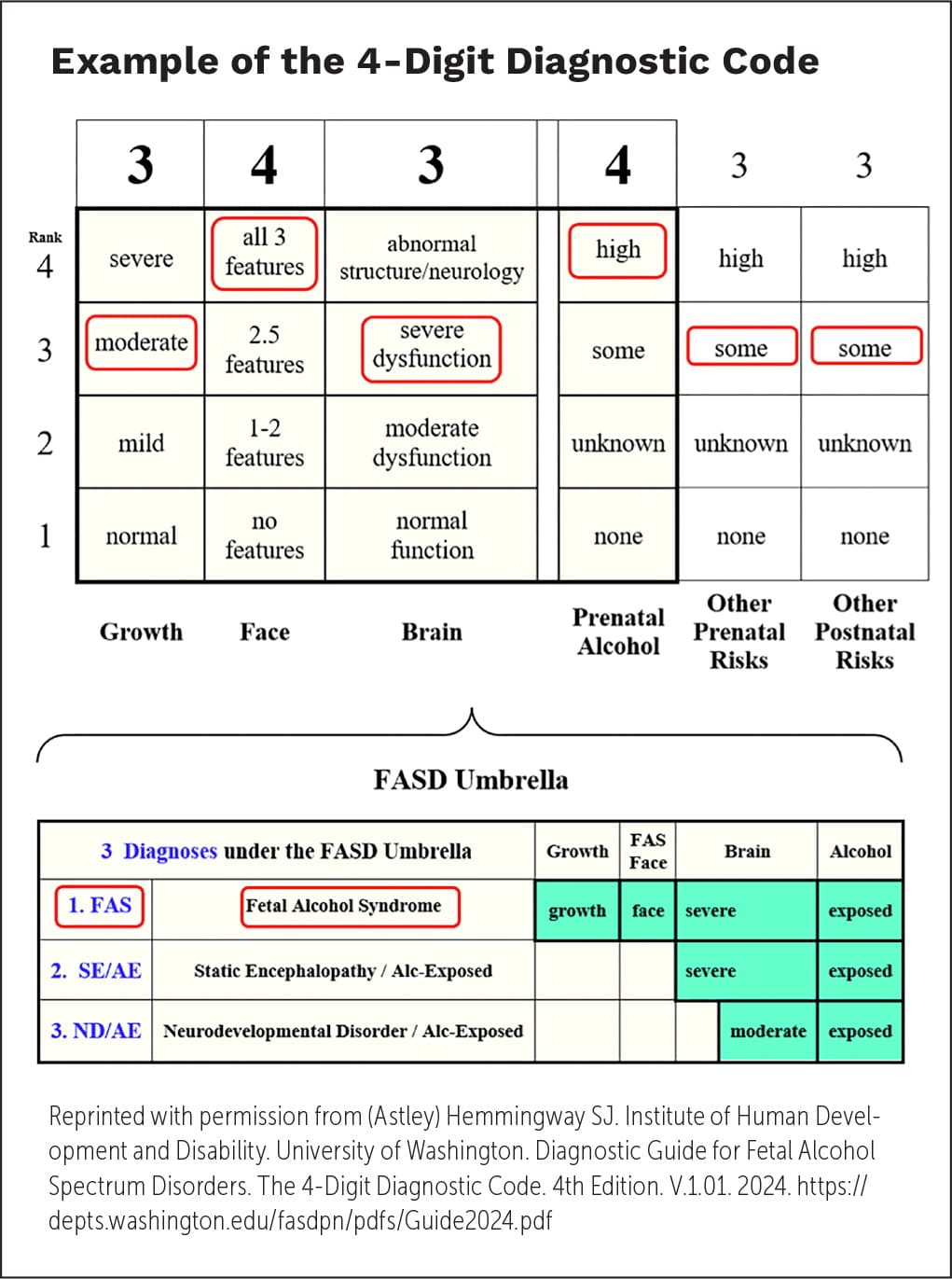
Reprinted with permission from (Astley) Hemmingway SJ. Institute of Human Development and Disability. University of Washington. Diagnostic Guide for Fetal Alcohol Spectrum Disorders. The 4-Digit Diagnostic Code. 4th Edition. V.1.01. 2024. https://depts.washington.edu/fasdpn/pdfs/Guide2024.pdf
FASDs 4-Digit Diagnostic Code
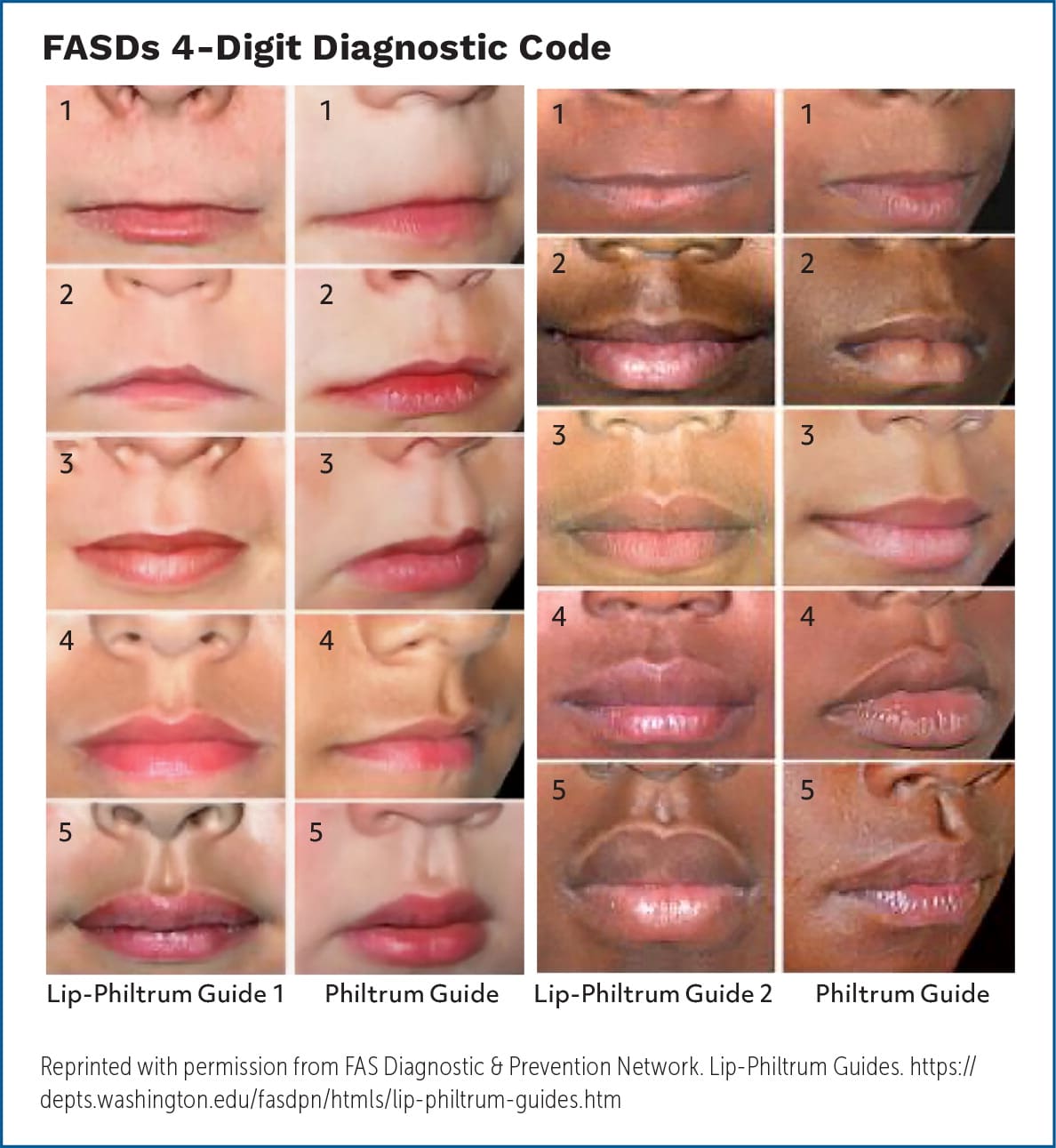
Reprinted with permission from FAS Diagnostic & Prevention Network. Lip-Philtrum Guides. https://depts.washington.edu/fasdpn/htmls/lip-philtrum-guides.htm
Treatment
While there are no cures and medications approved for the treatment of FASDs, early detection and interventions can significantly improve long-term outcomes and reduce symptoms, and secondary conditions can be treated. Long-term interventions can improve outcomes and include a holistic package of the following20,21:
- Adaptive functioning and educational interventions aimed at language attainment, math skills and safety.
- Psychosocial interventions and social skills training to address impulse control, attention and communication.
- Nutritional support to address common malnutrition, vitamin deficiencies, growth deficits and household food habits.
- Behavioral health care, case management, play therapies and ongoing identification of disorders.
- Parental training and family support to address common home instability issues, substance use, child discipline methods and parental support groups.
- Pharmacologic interventions to treat the range of cooccurring mental and behavioral health diagnoses, like alpha-2 adrenergic agents, selective serotonin reuptake inhibitors, mood stabilizers, stimulant and non-stimulant ADHD agents, and antipsychotics.15
- School-based accommodations such as individualized learning plans and counseling.
- Civil and criminal justice system advocacy.
- Strengths-based emphasis on the care of FASDs, which is less stigmatizing and more effective in empowering patients.
Resources
The American Academy of Family Physicians (AAFP) has developed many resources and CME offerings that address substance misuse and excessive alcohol use, along with specific resources addressing FASDs.
- Addressing Alcohol and Other Substance Use Practice Manual (www.aafp.org/dam/AAFP/documents/patient_care/alcohol/alcohol%20practice%20manual%202023.pdf)
- Training and Resources Related to Alcohol and Other Substance Use During Pregnancy (www.aafp.org/dam/AAFP/documents/patient_care/alcohol/training%20and%20resources%20related%20to%20alcohol%20and%20other%20substance%20use.pdf)
- Reimbursement and Coding for SBIRT Services (www.aafp.org/dam/AAFP/documents/patient_care/alcohol/reimbursement%20and%20coding%20for%20sbirt.pdf)
- Fetal Alcohol Spectrum Disorders. Free Online CME (www.aafp.org/cme/all/child-adolescent-health/fasd.html)
- Addressing Prenatal Alcohol and Other Substance Use. Free Online CME (www.aafp.org/cme/all/maternity/addressing-prenatal-alcohol-and-other-substance-use.html)
The American Academy of Pediatrics FASD Toolkit maintains a collection of resources on FASDs to support pediatricians, non-physician clinicians and allied health professionals.
- Fetal Alcohol Spectrum Disorders (www.aap.org/fasd)
These CDC repositories contain useful information and links to additional resources.
- Fetal Alcohol Spectrum Disorders (FASDs). About FASDs (www.cdc.gov/fasd/)
- About Alcohol Use During Pregnancy (www.cdc.gov/alcohol-pregnancy/about/index.html)
The Collaborative Initiative on Fetal Alcohol Spectrum Disorders (https://cifasd.org) informs and develops effective interventions and treatment approaches for FASDs through clinical and translational research.
FASD United provides resources and programs to individuals living with FASDs, their families, caregivers and supporters with expert, confidential support and referrals.
- The FASD Family Navigator (https://fasdunited.org/family-navigator/) serves members of the community with FASDs with connections to one-on-one support, referrals to resources and services, information about prenatal alcohol exposure and questions about FASDs.
- Resource Directory (https://fasdunited.org/resource-directory/) provides resources for individuals and families affected by FASDs.
The FAS Diagnostic & Prevention Network
- Online Course: (2024) FASD 4-Digit Diagnostic Code (https://depts.washington.edu/fasdpn/htmls/online-train.htm)
- Diagnostic Guide for Fetal Alcohol Spectrum Disorders. The 4-Digit Diagnostic Code (https://depts.washington.edu/fasdpn/pdfs/Guide2024.pdf)
The Substance Abuse and Mental Health Services Administration maintains the drug and alcohol treatment programs directory, called FindTreatment.gov (www.findtreatment.gov).
The National Institute on Alcohol Abuse and Alcoholism helps adults find alcohol treatment for themselves or an adult loved one through the Treatment Navigator (https://alcoholtreatment.niaaa.nih.gov).
