
From "the four most important words in medicine" to "the one question you should never ask your patients," these lessons can help you avoid pitfalls and experience more joy in practice.

I recently retired after 32 years of practicing family medicine, including caring for patients in the office, hospital, nursing home, urgent care, and obstetric settings and teaching physicians, residents, and students. Over the years, I have collected a number of “pearls” — small but valuable lessons learned through experience and struggle. Previously in FPM, I shared coding and documentation pearls.1–2 In this article, I'll share practical pearls that can help you care for patients, stay out of trouble, and avoid burnout.
KEY POINTS
- Small shifts in how you communicate with patients can affect their satisfaction. For example, if you happen to be running behind, “Thank you for waiting” sets a more positive tone than “Sorry I'm late.”
- To avoid running behind, aim to work at 90% to 95% of your maximum capacity. This leaves room in your schedule for last-minute patients, committee work, EHR work, or learning new skills.
- Other keys to an efficient and rewarding practice include hiring a good nurse (or MA), always having a follow-up plan, identifying your preferred workflows, and understanding your work RVUs.
1. REMEMBER THE FOUR MOST IMPORTANT WORDS IN MEDICINE: “THANK YOU FOR WAITING.”
Imagine this scenario: You are running behind schedule, and an emergency crops up or a complex visit slows you down. Now you are running way behind. You enter the next exam room, and you see a frown. The patient is staring at their watch. You then smile and say the four most important words in medicine — “Thank you for waiting” (which is more positive than saying “Sorry I'm late”). You see their frown soften as you give a quick explanation: “I just admitted a patient to the hospital” or “I had to address some major concerns this morning.” The patient smiles and responds, “I understand.” With four simple words, you have turned a potentially mad patient into an understanding patient, and you can now begin the visit on the right foot.
This approach works even better if you also sit down when you enter the exam room, signaling to the patient that you are not rushed and are focused on them.3 And, of course, the best situation is to not be running behind at all because you're working at 90% to 95% of maximum capacity (more on that later).
2. DON'T ASK “WHAT BRINGS YOU HERE TODAY?”
Some doctors' standard opening line to patients is “What brings you here today?” Their intent is to elicit the patient's concerns, but some patients take this to mean that the doctor hasn't looked at their chart and does not know what is going on with them. The patient has likely already told the scheduler, the front-desk staff, and the nurse or medical assistant the reason for their visit, so they expect their physician to be ready to discuss it, not ask them to repeat it. As the Boy Scouts say, be prepared. Always review the chart before seeing the patient, and show that you're prepared to address their specific concerns.
3. ADD VALUE TO THE VISIT
You see a patient for a new dark, irritated skin lesion. As soon as you walk into the exam room, you know it is a classic seborrheic keratosis. You can respond in one of two ways.
Option 1. You take a quick look and say, “It's benign. Don't worry about it.” Time spent: 1–2 minutes. Result: The patient may feel embarrassed for coming in for what she is told is a trivial concern or may feel angry about the short visit and wonder if you took her concern seriously.
Option 2. You examine the skin, looking for other lesions. You discuss seborrheic keratosis and offer cryotherapy treatment if indicated (explaining that insurance usually does not cover it for cosmetic reasons but may cover it if the skin is irritated or inflamed). You discuss red flags for skin cancer and sun avoidance/skin protection, and you supplement this advice with a patient information handout. You thank the patient for bringing any concerning skin changes to your attention and validate her concerns. Time spent: 8–10 minutes. Result: The patient leaves your office reassured that she does not have melanoma.
It does not take a lot of extra time or effort to add value to the visit.
4. ALWAYS COMMUNICATE THE FOLLOW-UP PLAN
A patient saw Doctor A for a problem. The problem did not improve with the initial treatment, so the patient fired Doctor A and is now seeing Doctor B because the first doctor “did not help me.”
In addition to diagnosing the problem, educating the patient, and developing a treatment plan, don't forget to discuss the follow-up plan. Always tell the patient what to do if the problem doesn't improve. Discussing what to expect, when to come back, and what your next plans are if the problem does not get better helps the patient understand that you have more options to help them. For example, “Let's try the simple things first, and then if you do not improve, we may need to do X” — start a medication, begin physical therapy, order an X-ray, etc.
5. “NEVER WORRY ALONE.”
When faced with a patient who has concerning symptoms and an elusive diagnosis, “never worry alone.” This medical saying means it is time to get a second set of eyes on the patient — via consultation or referral. While waiting for the consultation or referral, do not delay your own appropriate, aggressive workup of the patient.
6. FIND A GREAT OFFICE NURSE (OR OTHER CLINICAL SUPPORT STAFF)
One of the most important decisions you will make in practice is finding a great office nurse (or medical assistant [MA], if that's the norm in your practice). All the great doctors I have known have had great nurses, and many of them have worked with the same one for the majority of their career. Even if you are not the practice owner but an employee, you should still have input in choosing your nurse or other clinical support staff. If you are starting a new practice, put the word out to physicians, nurses, and staff that you are looking for a great office nurse. When starting with a new nurse or MA, consider a one- to two-month trial period, if possible.
A great nurse is someone who cares deeply about their patients. They have the ability to anticipate what needs to be done and do it before being asked, are always prepared, and act professionally. They show kindness to all, firmness when needed, and calmness even during emergencies. They possess excellent communication skills. They help address the patient's concerns and never pass the patient off to someone else. In contrast, imagine working with someone who is always late, brings drama to the clinic, is disrespectful, is not helpful to patients on the phone, and is hard to find when you need them.
Once you have found that great nurse or MA, acknowledge that you are a team, working together to provide great care to “our” patients, not “my” patients. Their dedication and hard work play a big part in your success as a physician, so recognize that in both tangible and intangible ways, such as excellent pay and appreciation.
7. IDENTIFY YOUR BEST PRACTICES — AND MAKE SURE YOU FOLLOW THEM
Within a very short time of starting practice, you will find patient care routines and workflows that work best for you. Here are some examples:
- Whether you want the patient's blood drawn before or after the visit,
- What problems you will see and what problems you will typically refer,
- What problems require an office visit and what problems you will manage with an e-visit or over the phone,
- How you will handle patients seeking narcotics,
- Scheduling preferences,
- What types of patient messages require your attention or can be handled by staff.
As you identify your best practices, educate your clinical support staff on how they can implement them. Being clear about what you want and giving them permission to carry out these tasks (within their scope of practice) will cut down on them asking you the same questions over and over again. However, for this to work, you need to be consistent and follow your own rules. Don't be rigid, but don't constantly be making exceptions either.
8. WELCOME PATIENTS' LISTS — AT THE RIGHT TIME
Do not address patients' lists during annual exams. Looking back, one of my biggest mistakes when starting medical practice was not educating my patients that their annual exam is for addressing their chronic medical concerns, medications, lab work, health maintenance, etc. While it is reasonable to address one or two minor acute problems as well, some patients come to the annual exam with a long list of new significant problems that have been brewing over the past 11 months and expect you to address them all at this one visit.
Annual exams already take longer than regular office visits. If you start addressing a long list of new problems, annual exams can become unmanageable. If I were starting over, I would educate my patients to come in and see me as acute problems arise and not to save them up for their annual exam.
At regular office visits, I always welcomed patients' lists. When patients would write out their symptoms, I found that it helped them more clearly communicate their concerns and sped up history taking. So, embrace the patient list. If appropriate, address all problems at that visit. For patients with complex or multiple problems, explain that it may take more than one visit to address them fully. If the patient is experiencing a major problem (e.g., severe depression or chest pain), address that problem first and save the other concerns for another visit. (For more on patient lists, see “Five Steps to Mastering Agenda Setting,” FPM.)
9. FIND THE PROPER MIX OF PATIENT VISITS FOR A MANAGEABLE SCHEDULE
Certain types of visits take more time (consults, physicals, new patients establishing care, new onset depression, procedures, etc.). And certain patients take more time. For example, you know when you see Mr. Jones that the visit is going to take twice as long as a normal visit no matter how hard you try to move things along.
How do you address the patients and visit types that take extra time? You have two options:
- Make that patient visit or visit type longer (e.g., 30-minute visits for new patients establishing care instead of 20-minute visits),
- Limit the number of times per day you will offer certain visit types (e.g., a max of three annual exams in the morning and three in the afternoon).
For new physicians starting practice, it may take a few months to see where the roadblocks are developing and adjust your schedule accordingly. Some health systems do not allow physicians to fine-tune their schedules, but you should advocate for it. When physicians have poor control over their schedules and other aspects of their work, they are more likely to experience burnout, reduce clinical effort, or leave their organization.4 A schedule filled with long, complicated visits can put you on the fast track to burnout and leaves no time in the schedule for simple acute visits or quick rechecks.
10. DON'T WORK BEYOND YOUR MAXIMUM CAPACITY
When we work at 90% to 95% of our maximum capacity by right-sizing our patient panel,5 our practice is more likely to run smoothly and our patients are more likely to receive excellent care. In turn, we can get home on time and spend minimal time after hours or on weekends doing catch-up work.
What also happens when we find this “sweet spot” is that we are more efficient at work. We can fit in that patient who calls or walks in and needs to be seen. We can see that second child when Mom says, “Michael's ear is also hurting. Could you see him too?” We are more apt to volunteer our expertise on hospital and clinic committees to improve patient care. We can show up fully and contribute to our department meetings. Our positive attitude rubs off on the staff, residents, students, and patients we interact with. Our positive outlook makes us the ideal recruiters for new partners. We have time to learn how to document and code correctly and to become experts in using our EHR. We have time to learn new skills and procedures and go to conferences. And sometimes we even have time to see patients on our afternoon off because we aren't burned out.
What happens when we chronically work beyond our maximum capacity? Everything breaks down, including our eating habits, sleep, daily exercise, and home life. At work, we skip lunch or take a quick lunch break at our desk. We feel relieved when a patient doesn't show because it gives us time to catch up. We want to stop taking call. We start limiting our scope of practice. We stop teaching medical students and residents. We quit going to department meetings and serving on committees. Our patients and coworkers sense our negative attitude, and we become poor recruiters for our clinic and department. We become less efficient and less happy.
Closing your practice to new patients when it becomes full, right-sizing your patient panel, and fine-tuning your schedule can all help you find the sweet spot. If your organization's leaders do not allow this, they are contributing to physician burnout and attrition.4
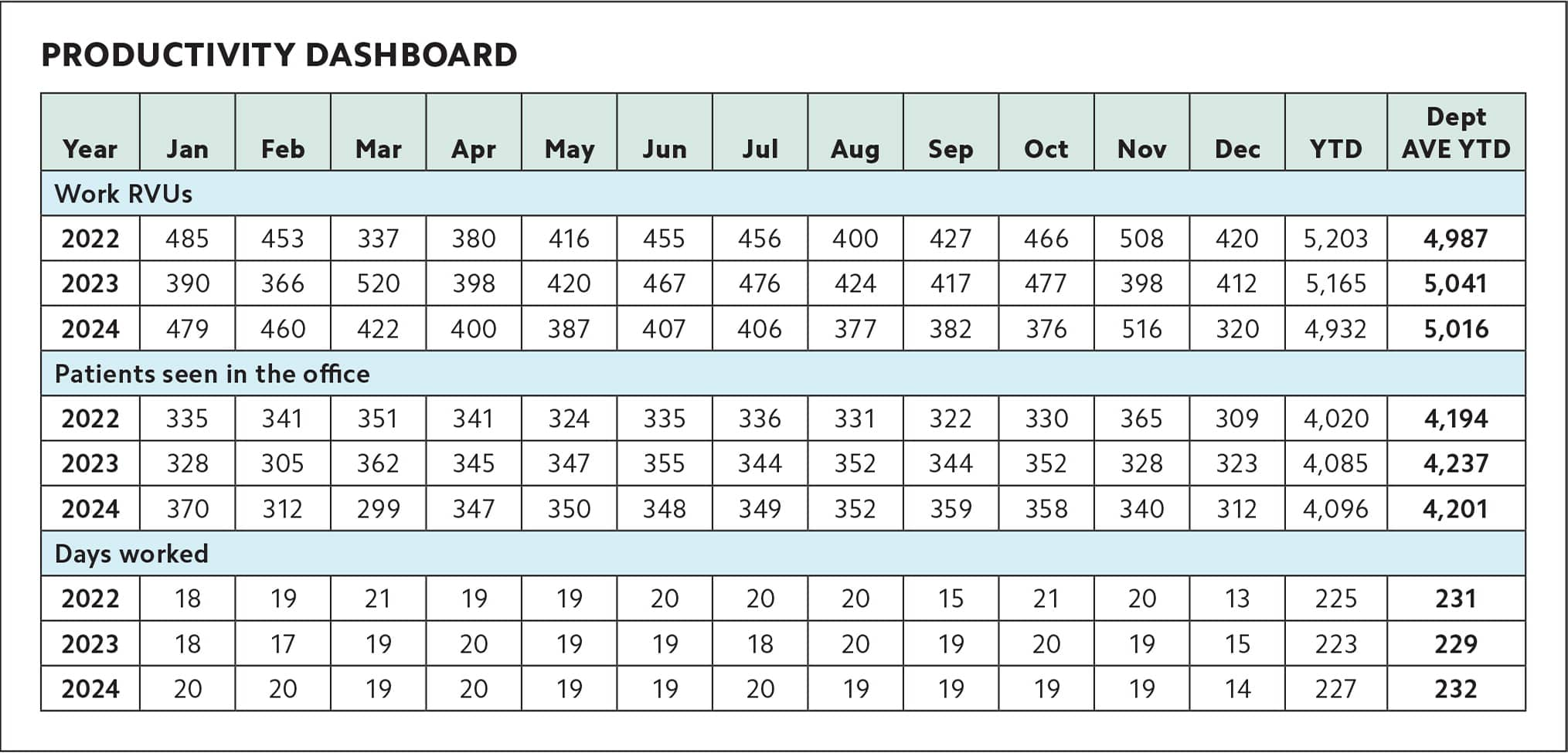
11. TRACK YOUR PRODUCTION WITH A DASHBOARD
Can you view your entire work/production history on a single page? Yes, you can. I call it “the better dashboard.” To create this simple dashboard, have your clinic or health system track the following metrics:
- Your billings or work relative value units (RVUs) per month, depending on how you are paid,
- Your number of patients seen in the office per month (or in the hospital if you are a hospitalist),
- Your number of days worked per month.
Include your yearly totals and your department average, if desired, so you can see how you are doing year over year and how you compare with the rest of your department. You will likely find that your production varies month to month but is fairly consistent year to year, unless you had a major change in practice. If you see something that does not make sense, such as a drop in work RVUs, figure out why it occurred. Did you take more time off than usual? Did your practice change coders? Did your production change because you're doing fewer procedures or more preventive care? Did your duties change (e.g., you started seeing nursing home patients or you stopped hospital work)? You need to know how these changes are affecting your production because it affects your compensation.
PRODUCTIVITY DASHBOARD
| Year | Jan | Feb | Mar | Apr | May | Jun | Jul | Aug | Sep | Oct | Nov | Dec | YTD | Dept AVE YTD |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Work RVUs | ||||||||||||||
| 2022 | 485 | 453 | 337 | 380 | 416 | 455 | 456 | 400 | 427 | 466 | 508 | 420 | 5,203 | 4,987 |
| 2023 | 390 | 366 | 520 | 398 | 420 | 467 | 476 | 424 | 417 | 477 | 398 | 412 | 5,165 | 5,041 |
| 2024 | 479 | 460 | 422 | 400 | 387 | 407 | 406 | 377 | 382 | 376 | 516 | 320 | 4,932 | 5,016 |
| Patients seen in the office | ||||||||||||||
| 2022 | 335 | 341 | 351 | 341 | 324 | 335 | 336 | 331 | 322 | 330 | 365 | 309 | 4,020 | 4,194 |
| 2023 | 328 | 305 | 362 | 345 | 347 | 355 | 344 | 352 | 344 | 352 | 328 | 323 | 4,085 | 4,237 |
| 2024 | 370 | 312 | 299 | 347 | 350 | 348 | 349 | 352 | 359 | 358 | 340 | 312 | 4,096 | 4,201 |
| Days worked | ||||||||||||||
| 2022 | 18 | 19 | 21 | 19 | 19 | 20 | 20 | 20 | 15 | 21 | 20 | 13 | 225 | 231 |
| 2023 | 18 | 17 | 19 | 20 | 19 | 19 | 18 | 20 | 19 | 20 | 19 | 15 | 223 | 229 |
| 2024 | 20 | 20 | 19 | 20 | 19 | 19 | 20 | 19 | 19 | 19 | 19 | 14 | 227 | 232 |
12. WORK IN “SUNSHINE ROOMS” AND KEEP A “SUNSHINE FILE.”
The term “sunshine file” describes a file or folder of all the letters, cards, and notes of gratitude you have received from your patients over the years. On tough days, you can use this file to cheer yourself up.
I have never had to use my sunshine file because I turned my exam rooms into “sunshine rooms.” When I started practice, I began making bulletin boards containing Polaroid photos of all the babies I delivered (or cared for) when they turned four months old and all my patients when they turned 80. I also included anniversary and graduation announcements and other patient milestones. No one declined having their picture taken, because everyone considered it an honor to be on one of the bulletin boards. It was a sad day many years ago when I removed all 75 bulletin boards to paint the walls.
Some physicians work in the same offices and exam rooms for years and yet spend zero time, money, and energy decorating them. It doesn't take much. Think about what's important to you and what you wish to share with your patients. Then add some photos, mementos, artwork, or appropriate patient education posters to help personalize your work areas so they are bright, interesting, pleasing to the eye, and mood-lifting.
EXPERIENCING MORE JOY IN MEDICINE
Family medicine is a rewarding career, but it is also challenging. “The days are long, but the years are short,” as they say. Before you know it, you'll stand where I stand, looking back at decades of patient care. I hope these pearls6 can help you experience more joy in practicing medicine, as they did for me.
