
Having a team member whose time is split 50-50 between inbox cross coverage and acute care can reduce physician burden while increasing patient access.

According to a 2023 Medscape report, 57% of family physicians say they are burned out, with “bureaucratic tasks” and the “increasing computerization of practice” most frequently cited as the causes.1 We now use terms like “pajama time” to describe the hours we spend in our EHR after leaving the clinic, charting the day's patient visits and tending to a seemingly bottomless inbox of messages, correspondence, and forms.2 When a colleague is out of the office on vacation, leave, or the inpatient service, the task of monitoring their unattended inbox adds to the burden of addressing our own. Previous articles have proposed inbox management solutions, including using clinic staff to triage messages so physicians only have to address those that truly need their attention.3–6 These strategies have merit, but the volume of messages and high rates of burnout persist.
Our organization addressed this problem by creating a new role: the 50-50 inbox clinician (IC) — a nurse practitioner or physician assistant who spends half their time performing inbox cross coverage and the remainder of their time seeing patients for acute care, which funds their salary.
KEY POINTS
- An “inbox clinician” (IC) who spends half their time on inbox cross coverage can offset their salary and benefits by spending the other half seeing acute care patients.
- An IC can alleviate physicians' inbox burden, in part by managing urgent messages and being the go-to resource for nursing staff.
- Things to consider before implementing an IC include how many inboxes they will cover, whether they will be allowed to work remotely while covering inboxes, and what timelines to establish for ICs to handle common types of messages.
THE INTERVENTION: THE INBOX CLINICIAN
Our purpose in creating the IC role was to disrupt the status quo by designating a single licensed clinician to take on urgent messages, provide scheduled inbox cross coverage for colleagues who are out of the office, and be the go-to resource for nursing staff (who do the initial triage of messages) so they don't have to track down the other clinicians. Our goal was to reduce burnout among our clinicians and hopefully prevent some emergency department (ED) and urgent care visits for our patients.
For our initial IC pilot, we used funds our practice earned through value-based payment work to hire a nurse practitioner. We decided this clinician would have no patient panel of their own but instead would expand our same-day and next-day access by seeing patients for acute issues. To continue beyond the pilot period, we knew we would need to demonstrate financial sustainability. (See our results below.) At a second site, our residency practice, we jointly onboarded two full-time ICs with mirrored schedules (e.g., when one is seeing patients, the other is providing inbox cross coverage). Because of the different payment models at the two sites, the IC at the first practice had more flexibility in their inbox-time-to-patientcare ratio, whereas those in the second practice were held to a 50-50 model as we monitored their financial viability. (See “Clinic demographics”.)
CLINIC DEMOGRAPHICS
Clinic 1: Lone Tree primary care
- 1 inbox clinician
- 13 physicians, 4 advanced practice providers
- Clinicians per half day in clinic: 7–9
- Typical visits per half day: 49
- Hospital outpatient department — offsite, part of a remote “medical campus”
Clinic 2: AF Williams
- 2 inbox clinicians
- 26 faculty physicians, 20 resident physicians, 5 advanced practice providers (all are part-time)
- Clinicians per half day in clinic: 9–10
- Typical visits per half day: 55
- Hospital outpatient department — offsite, part of a remote “medical campus”
Having one practice with a single IC and another with dual ICs provided useful lessons about how to adapt the model. Depending on your local preference, a practice with two ICs can allow them to alternate duties day to day or week to week (e.g., one week of inbox management followed by one week of clinical care). This allows more flexibility for ICs to complete their inbox work remotely, which can help with recruitment. At our practice with one IC funded through value-based care revenues, that person must cover inboxes every day the clinic is open, devoting a half day to that and a half day to clinical care. This makes remote inbox work more challenging, especially if the IC has a long commute. With only one IC, it is also critical to create a backup inbox cross coverage system for when your IC is sick or on vacation themselves. In our organization, primary care clinicians seek IC coverage using a request system that the office managers of each clinic review. This system is subject to limitations on the total number of clinicians the ICs can cover on a given day and the total number of days per year allocated to each clinician.
In our practices, we offer each primary care clinician 28 days of IC inbox coverage per year. On any given day, the IC covers inboxes for three or four total full-time equivalent (FTE) clinicians (if multiple part-time primary care clinicians sign up, the IC may therefore cover more than four inboxes). Other practices can modify this to fit their needs (some may have more robust portal message usage per clinician than others). Each practice also must consider how they will manage high-demand times of the year, such as holidays (e.g. first-come, first-served vs. request system).
CHALLENGES TO IMPLEMENTATION
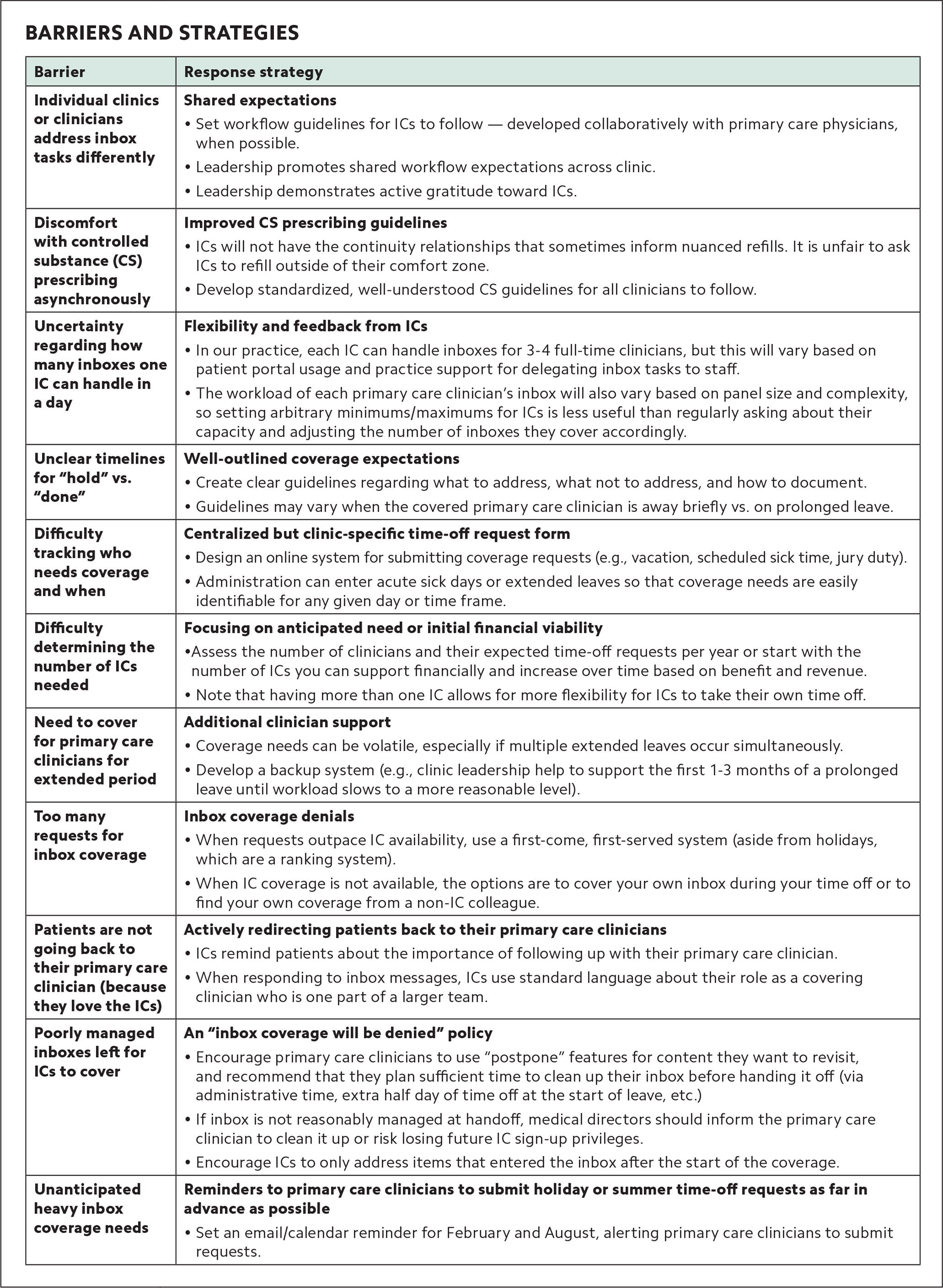
Our clinics identified and tackled barriers to implementation as they arose. Key challenges included inconsistent inbox expectations and workflows, discomfort with controlled substance prescribing outside a continuity relationship, and uncertainty around how many inboxes one IC could reasonably cover. (See “Barriers and strategies.”)
| Barrier | Response strategy |
|---|---|
| Individual clinics or clinicians address inbox tasks differently | Shared expectations
|
| Discomfort with controlled substance (CS) prescribing asynchronously | Improved CS prescribing guidelines
|
| Uncertainty regarding how many inboxes one IC can handle in a day | Flexibility and feedback from ICs
|
| Unclear timelines for “hold” vs. “done” | Well-outlined coverage expectations
|
| Difficulty tracking who needs coverage and when | Centralized but clinic-specific time-off request form
|
| Difficulty determining the number of ICs needed | Focusing on anticipated need or initial financial viability
|
| Need to cover for primary care clinicians for extended period | Additional clinician support
|
| Too many requests for inbox coverage | Inbox coverage denials
|
| Patients are not going back to their primary care clinician (because they love the ICs) | Actively redirecting patients back to their primary care clinicians
|
| Poorly managed inboxes left for ICs to cover | An “inbox coverage will be denied” policy
|
| Unanticipated heavy inbox coverage needs | Reminders to primary care clinicians to submit holiday or summer time-off requests as far in advance as possible
|
Implementing an IC is a relatively high-touch process. Onboarding the ICs, educating staff and other clinicians, gathering feedback, and making improvements required significant time from supervisors. One key area we had to monitor and make adjustments for was the ICs' clinical time. At one site, we reduced the IC's number of visits per session from 11 patients to eight to account for a greater-than-expected average length of visit due to the IC's lack of a continuity relationship with the patients as an unempaneled clinician and the complexity of patient needs (our call center protocols did not allow us to limit same-day access to simple acute needs).
We also found that as our IC program became the standard way of covering clinicians' inboxes, they quickly forgot the process for cross coverage when the IC was unavailable. Practices implementing a similar IC program may want to communicate contingency processes so clinicians can more easily recall expectations for this. In one of our practices, the physicians were so grateful for inbox coverage that the ICs became reluctant to request their own time off. We addressed this by having one-on-one meetings where we emphasized our backup coverage plans and encouraged them to take time off.
OUR RESULTS
Anecdotally, primary care clinicians at our sites who received inbox coverage voiced strong support for the IC program. We also heard positive feedback from medical directors who oversee these programs. Since launching IC programs at our first two clinical sites, we have placed ICs in two additional locations and, at the time we submitted this manuscript, were recruiting an IC for a fifth site.
At the residency practice, we conducted a pre-intervention survey and six-month post-intervention survey of all primary care clinicians (response rates were 75% for the pre-intervention survey and 65% for the post-intervention survey). There was no statistically significant difference for the single-item burnout question (“Based on your definition of burnout, how would you rate your level of burnout?”),7 with 44.7% of respondents reporting no or very little burnout pre-intervention and 50% reporting no or little burnout post-intervention. However, there was some indication that the intervention reduced inbox burden for the group of clinicians that had been feeling the most strain. In the pre-intervention survey, primary care clinicians who responded that they were considering lowering their clinical time (cFTE) because of inbox burden were considering lowering it by an average of 0.15 cFTE. In the post-intervention survey, that fell to 0.07 cFTE, which correlates with an estimated 3,168 annual patient visits retained across 12 post-intervention survey respondents.
After one year in practice, the financial analysis of the two ICs whose salary and benefits were paid for entirely by our organization's Department of Family Medicine showed they appeared to break even when seeing 7.2 patients per day. Accordingly, we have budgeted for eight patients per day. This break-even point is influenced by many variables, including individual billing practices and salaries.
IMPLEMENTATION GUIDANCE
To implement an IC in your practice, you will need to consider the following:
How much inbox coverage does your practice need? Does your practice need inbox coverage every day of the week or just some days?
What is your model for financial viability? How much billable clinical care does the IC need to offset their inbox time? A 50-50 time split is a rough guide, but this may vary based on your payer mix, the complexity of the acute care visits your IC handles, and the salary range of nurse practitioners and physician assistants in your area. Some practices may also have value-based care contracts that allow the IC to offset some of their salary by positively impacting outcomes related to your value-based work (e.g. reducing ED utilization or increasing Medicare Annual Wellness Visit completion).
What will their inbox cross coverage time include? Will you use the IC to cover all messages for primary care clinicians on vacation, sick time, or other planned leaves? Or will you use the IC only for urgent inbox escalations, as decided by the clinical staff members who triage messages? Will the ICs provide support for all primary care clinicians or only those with full-time or near full-time clinical duties?
What will inbox cross coverage work-flow expectations be? What type of inbox items will your IC manage to completion, and which will require the patient's primary care clinician to review? How quickly will you expect your IC to resolve common inbox items, such as test results and prescription refill requests? We created a reference guideline with our organization's expectations (see “Inbox clinician cross-coverage workflow expectations”). We recommend that all clinicians agree on a shared expectation, rather than asking each IC to learn various clinicians' preferences. We also set the expectation that each clinician hand off an empty inbox to the IC at the beginning of the day.
What will triage escalation workflows be? ICs can assist nurses and other clinic staff with time-sensitive items that require clinician-level review. Because the IC program's funding in one of our practices is linked to the prevention of unnecessary ED visits, that IC prioritizes assisting nurse triage with ED/urgent care disposition. ICs can also convert triage escalations to message appointments (online digital evaluation and management) or virtual visits to supplement their billable acute care work.
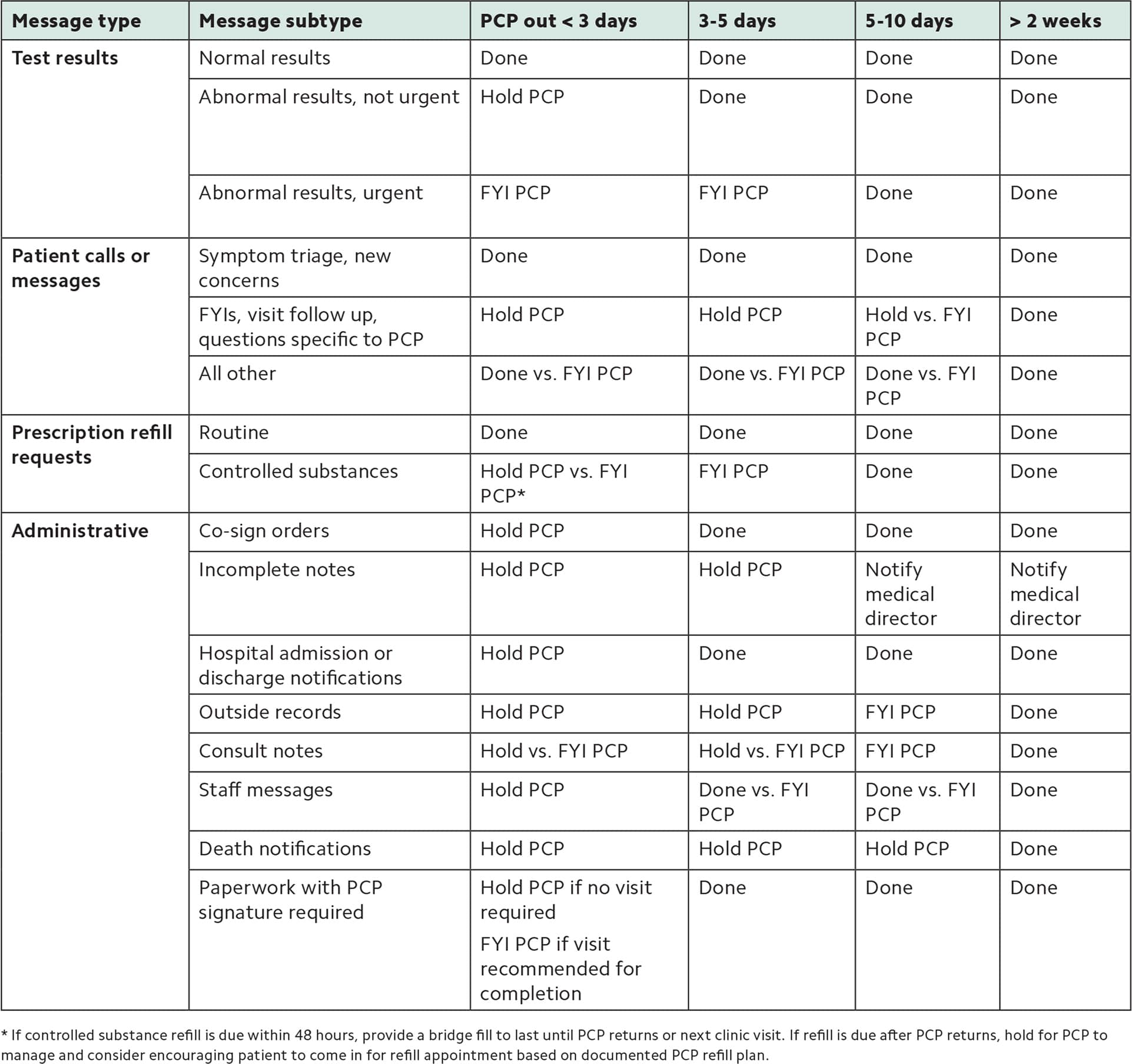
INBOX CLINICIAN CROSS-COVERAGE WORKFLOW EXPECTATIONS
Our guidelines for how inbox clinicians (ICs) handle messages depend on how long primary care physicians (PCPs) will be out.
- Done = IC manages to completion (responded/completed/removed from inbox).
- FYI PCP = IC handles message but leaves in inbox for PCP to review at their convenience.
- Hold PCP = IC does NOT handle message but tells the patient it will be addressed, leaves it in the inbox, and alerts the PCP to attend to it ASAP.
In some cases, the IC can choose between two actions (“vs.”) depending on individual patient circumstances.
| Message type | Message subtype | PCP out < 3 days | 3–5 days | 5–10 days | > 2 weeks |
|---|---|---|---|---|---|
| Test results | Normal results | Done | Done | Done | Done |
| Abnormal results, not urgent | Hold PCP | Done | Done | Done | |
| Abnormal results, urgent | FYI PCP | FYI PCP | Done | Done | |
| Patient calls or messages | Symptom triage, new concerns | Done | Done | Done | Done |
| FYIs, visit follow up, questions specific to PCP | Hold PCP | Hold PCP | Hold vs. FYI PCP | Done | |
| All other | Done vs. FYI PCP | Done vs. FYI PCP | Done vs. FYI PCP | Done | |
| Prescription refill requests | Routine | Done | Done | Done | Done |
| Controlled substances | Hold PCP vs. FYI PCP* | FYI PCP | Done | Done | |
| Administrative | Co-sign orders | Hold PCP | Done | Done | Done |
| Incomplete notes | Hold PCP | Hold PCP | Notify medical director | Notify medical director | |
| Hospital admission or discharge notifications | Hold PCP | Done | Done | Done | |
| Outside records | Hold PCP | Hold PCP | FYI PCP | Done | |
| Consult notes | Hold vs. FYI PCP | Hold vs. FYI PCP | FYI PCP | Done | |
| Staff messages | Hold PCP | Done vs. FYI PCP | Done vs. FYI PCP | Done | |
| Death notifications | Hold PCP | Hold PCP | Hold PCP | Done | |
| Paperwork with PCP signature required | Hold PCP if no visit required FYI PCP if visit recommended for completion | Done | Done | Done |
A WORTHWHILE INTERVENTION
For us, implementing an IC was a viable strategy to reduce inbox burden. While we did not see a significant decrease in overall burnout scores in our surveys, we did see a decrease in the amount of time by which clinicians were considering reducing their clinical hours due to inbox burden. In an environment in which it is often difficult to recruit and retain clinicians, this is a worthwhile investment, especially given that our ICs were revenue-positive additions to the team if they saw eight acute care patients per day.
