
An organized approach to quality improvement, with active physician engagement, led to an estimated 130 lives saved at 10 offices. Here's how they did it.

The prevalence of hypertension in the United States is staggering, with almost half of adults (119.9 million) meeting the American Heart Association's criteria for the condition — blood pressure (BP) ≥ 130/80 mm Hg or current use of medication to lower BP.1 Only about one-fourth of those (27 million) have their hypertension under control.1 Lowering BP significantly reduces cardiovascular (CV) events, stroke, and death with an absolute risk reduction of 28 CV events, 17 strokes, and nine deaths per 1,000 persons treated for five years.2
Due to its profound impact on outcomes, hypertension control is often a target for quality improvement (QI) and pay-for-performance programs. In 2021, our health care system was linking patient panel outcomes on certain quality measures, including hypertension control, to clinician performance pay. Unfortunately, many clinicians were skeptical of data accuracy and patient attribution, and they did not want to be held accountable for factors they could not control, such as medication adherence or measurements obtained in a different setting (e.g., the emergency department). In part because of these barriers, physician engagement in QI efforts was low across our 10 family medicine offices. Our rates of hypertension control were under target, and our approach to improvement was not yielding the desired results.
Recognizing the need for change, we began with the basics of quality improvement — identifying key drivers of hypertension control, developing a protocol with clear roles, defining leading measures, and rewarding our clinicians based on metrics they could understand and influence. After two years of sustained effort, we increased the absolute rate of BP control in our 10-practice family medicine department by 7.5%, to 78%. This exceeded the HEDIS top decile of 75.22% and translated to 1,445 more patients at goal. Using the conservative estimate of one death prevented for every 11 patients at goal over 10 years,3 this means about 130 lives would be saved over the next decade. (See the results.)
We are sharing our experience as a model for other practices to consider when implementing QI work around hypertension and evaluating quality performance incentives.
KEY POINTS
- Hypertension QI efforts should focus on key drivers of BP control such as BP measurement accuracy, timely follow up, and more aggressive advancement of pharmacotherapy.
- To ensure the team is on the same page, develop a protocol that clarifies the process or expectation for each of the key drivers (e.g., follow up with the patient within six weeks after an elevated BP).
- Build an incentive plan based on leading (process) metrics that clinicians can influence, not just lagging (outcome) metrics.
HOW WE DID IT
Our efforts to improve hypertension control spanned two years and included the following steps.
1. Identify key drivers. Researchers have identified several clinical barriers to hypertension control, including poor BP measurement technique4 and treatment inertia.5 Treatment inertia includes both failure to intensify treatment when indicated and failure to arrange timely follow up to reassess and further intensify as needed. Based on these principles, as well as the American Heart Association's “MAP” framework (measure accurately, act rapidly, and partner with patients),6 we identified the following key drivers of BP control:
- Measure BP accurately (proper in-office technique, confirmatory BP, and documentation),
- Act rapidly (appropriate diagnosis of hypertension, rapid follow up, and escalation of therapy),
- Partner with patients (home monitoring, case management, and patient education).
2. Develop a hypertension protocol. To make sure the entire team was on the same page, we realized we needed to develop a comprehensive protocol that a) addressed the key drivers in a practical manner and b) defined how each team member would contribute. We started with one of our family medicine residency offices. Its quality team, a multidisciplinary group of physicians, pharmacists, nursing staff, and administrative leadership, developed a protocol based on best practices and the most recent literature on antihypertensive medications. The protocol covered the following:
- Clinical intake, including who performs each step in the process and when and how to take a repeat BP reading,
- General medication and counseling guidance for clinicians,
- Advice about when and how to incorporate the clinical pharmacist,
- A recommended follow-up schedule (e.g., follow up with the patient within six weeks after an elevated BP).
After an initial launch of the protocol in the fall of 2021, we performed monthly audits to assess adherence in the pilot office. Given the high rate of disease and staffing demands, the team experienced many challenges, specifically with completing repeat BP readings. It took many audits, bidirectional feedback, and workflow efficiency training to get that specific step flowing well. Based on the pilot office's experience, we provided more automated measurement equipment and nursing support to our other locations as we pushed QI efforts department-wide.
We later revised the hypertension protocol with input from pharmacy and nursing leadership as well as a hypertension specialist. We were introduced to the HEARTS technical package, developed as part of the World Health Organization's Global Hearts Initiative,7 which has helped national health systems transform hypertension control rates through organized guideline development and monitoring. Using that program's experience, we incorporated two major areas to our protocol:
- A clear process for nonphysician follow-up visits (pharmacy or nursing),
- A clear guideline for advancing pharmacotherapy based on current best evidence.
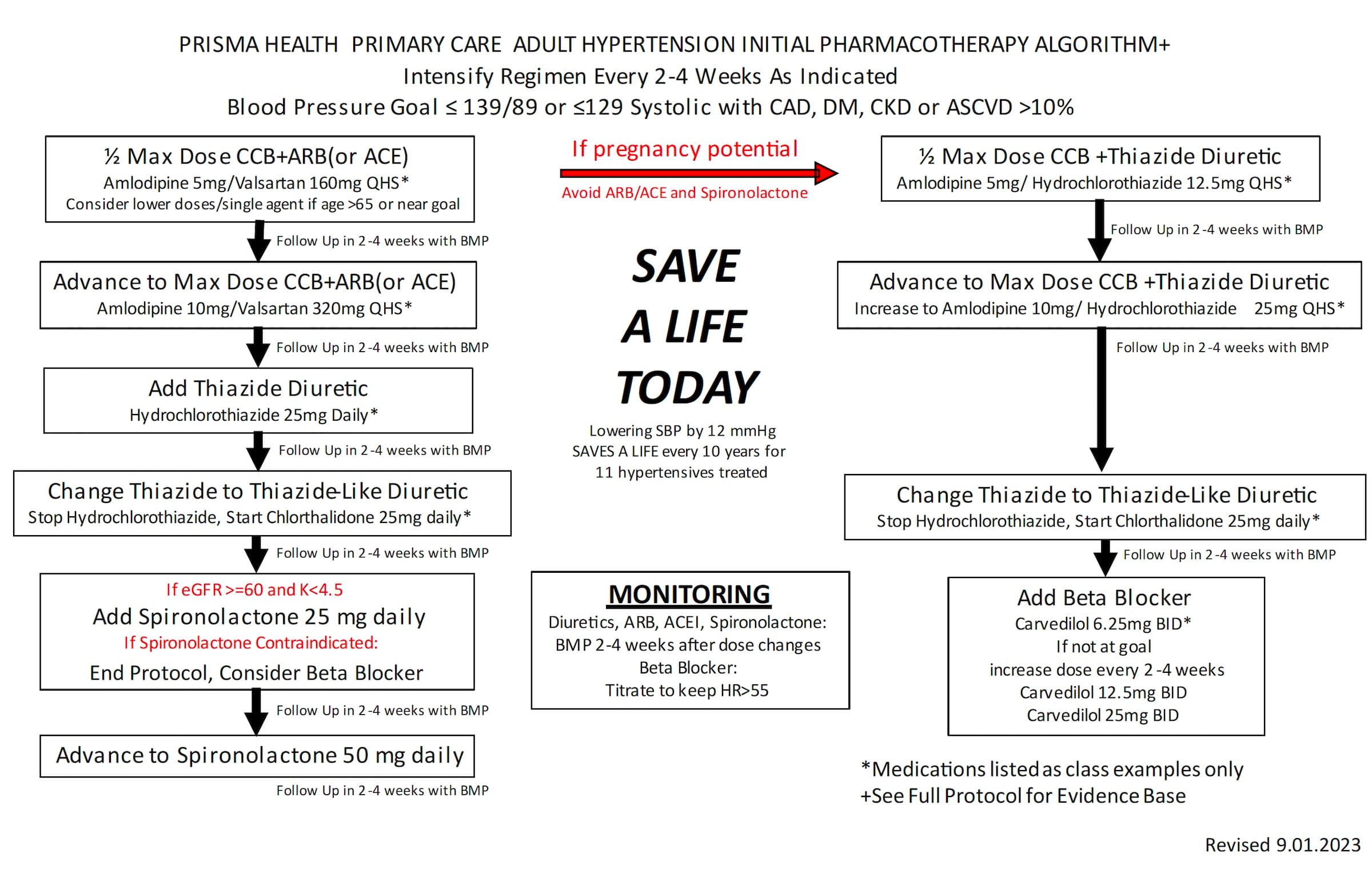
In addition to the hypertension protocol, we also created an algorithm for pharmacotherapy advancement and a guide for nurse-led BP visits. (See "Online tools.")
We launched the protocol department-wide in December 2022 via staff meetings, nurse training, a formal presentation to all clinicians, and ongoing support from clinical pharmacists and quality specialists. Our departmental physician leaders also visited each office to review the protocol with clinicians and highlight the expected reduction in patient mortality.
ONLINE TOOLS
Download the following tools as PDF documents:
3. Build an incentive plan based on leading metrics. A year before we launched our protocol, we had already made significant department-wide efforts around improving hypertension control, such as deploying additional automated measurement devices and investing in clinical team member training, as mentioned earlier. In April 2022, we launched an incentive plan for our clinicians based on metrics that a) addressed the key drivers of hypertension control and b) they could influence in their office by changing their personal practice or in partnership with their office team. We deliberately included “leading” (process) metrics not just “lagging” (outcome) metrics.
Our departmental leadership agreed on the following metric for weekly assessment of patients with hypertension who had been seen in the office:
(Number of patients with BP at goal + Number of patients with BP above goal and follow up scheduled in < 6 weeks) ÷ Total number of patients with hypertension seen in the office = Rate of hypertension control
This metric incentivized obtaining an accurate BP and using sequential measurements to obtain further readings, which normalized the findings about 30% of the time. It also promoted arranging close follow up, a marker for rapid intervention. Both aspects were achievable. Based on baseline performance, we picked a goal of 80%. Since the data was made available weekly, we gave clinicians the opportunity to “try again” within the same month, rewarding improvement in addition to baseline performance.
Our clinicians found it incredibly encouraging to be assessed based on factors they could control. They engaged with their data, trusted it, and helped produce it. They made changes to their personal practices and their teams' workflow, such as supporting their nurses in BP rechecks and creating more access for timely follow-up. They became invested in QI in a real and meaningful way. They also received support from a team of quality specialists from our larger network, who helped produce the metrics, performed chart audits, and provided technical support. While this quality team had been working with the sites all along, they became newly empowered because of the energy and interest from their clinician colleagues.
In September 2021, before starting the incentive program, 9 out of 36 clinicians in our offices hit the 90th percentile nationally in HEDIS for hypertension control. Eleven months later, 16 out of 36 clinicians had risen to that level. An additional 15 clinicians had improved by more than 10%, and the remaining 5 clinicians had at least achieved our departmental goal of 80%. Thus, we had 100% engagement in improving BP control, and all clinicians were able to receive financial incentives for the metric.
Although our health system paused its original incentive program in late 2022, our team was already engaged in the work. Seasoned physicians questioned newer aspects of the algorithm yet were ready to review the evidence, site managers tracked their intake metrics regularly, and we were all able to focus on what was most important — saving patients' lives. Our hypertension control rates continued to improve (see the results) even without that specific incentive, although the health system reincorporated the incentive in later years.
RESULTS
The graphs below show the six-week BP follow-up rate (the percentage of patients with BP above goal and follow up less than 6 weeks after an elevated BP) as well as hypertension control over time for our department (FM Midlands) vs. our sister department, which was not directly engaged in the QI efforts highlighted in this article. Overlayed are our departmental interventions as well as system-wide interventions. After two years of sustained effort, our rate of control increased 7.5% to 78%, exceeding the HEDIS top decile of 75.22%, translating to 1,445 more patients with a BP < 140/90 mm Hg and roughly 130 lives saved over the next decade.3 Our rate of improvement in both metrics significantly outperformed that of our sister department and was sustained through the study period.
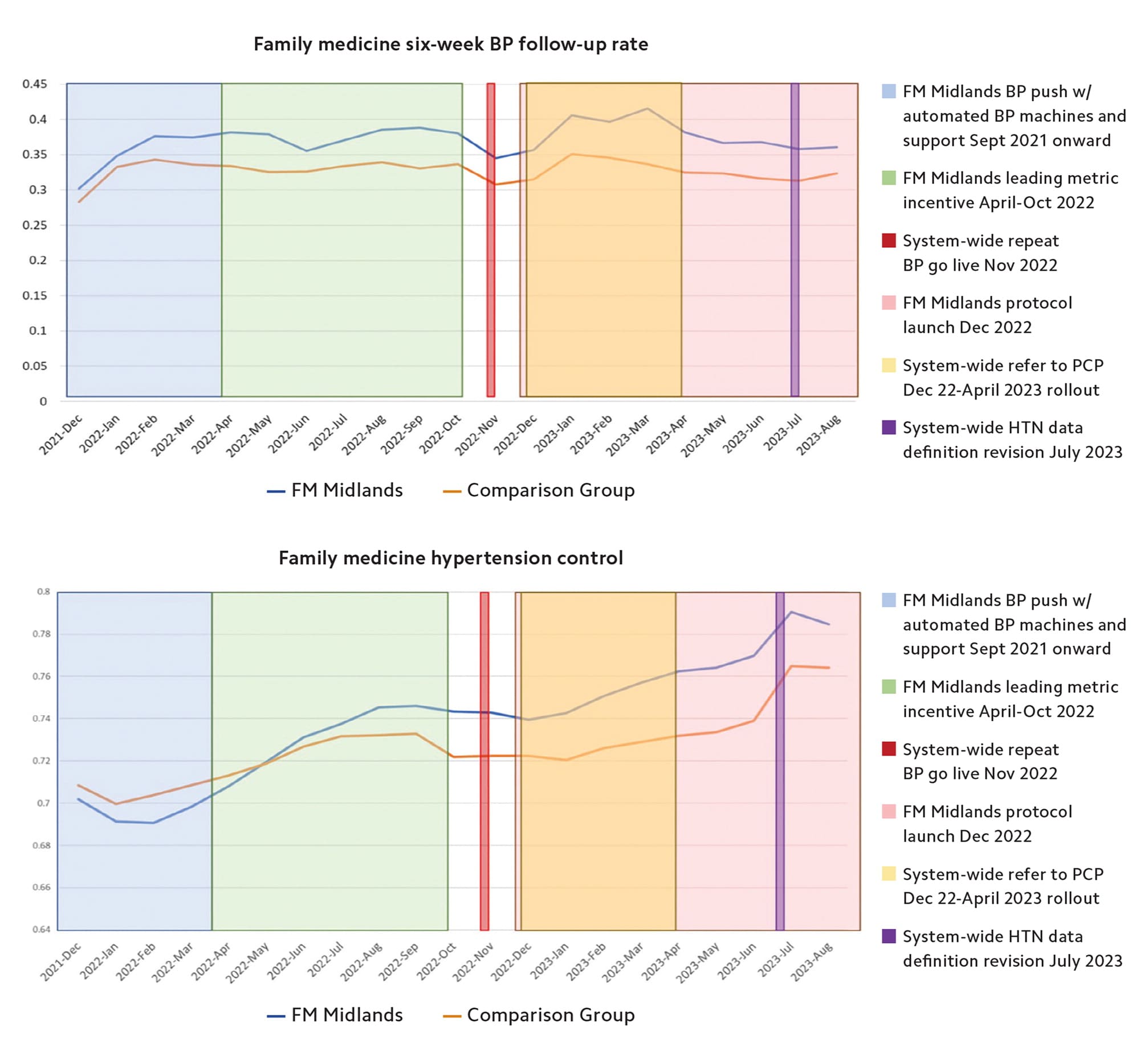
4. Incorporate system-wide interventions. Our 10-practice family medicine department (“FM Midlands”) is one of four primary care departments in a larger health care system (Prisma Health). In addition to our local departmental projects, there were system-wide interventions to address hypertension. These included new functions in our EHR promoting reassessment when BPs were elevated and referral to primary care when BPs were elevated in a specialty office. These changes affected care throughout the system.
LESSONS LEARNED
Creating behavior change is hard, and creating it within a busy clinical team is no exception. It is incredibly rewarding to look back on two years of organized efforts to improve hypertension control and see clinically significant changes in our practices. We offer the following reflections on the process:
Focus on patient care aspects you can control. We believe success lies in framing QI efforts as a means for providing excellent patient care, rather than hitting an externally established metric. Pivoting our incentive program from focusing on the overall BP control of a clinician's panel to their day-to-day practice performance was critical. It changed conversations almost overnight from arguments about attribution and blaming other specialties to goal-oriented questions about access, practical approaches to nurse-only BP visits, and workflow challenges. Making this change was not easy. It took strong leadership from our department chair to obtain approval of this customized approach in our large network, and it required significant data management each month to extract information from our EHR. This led to another benefit, as our practice managers gained EHR reporting and spreadsheet skills.
Welcome discussion. While the hypertension protocol we developed was evidence-based, we expected resistance from our clinicians. We purposefully engaged some of our most vocal team members early, involved representatives from all cadres within the team as well as experts in the field, and ensured all components of the guideline were based on patient-oriented evidence. We circulated drafts regularly to the leads of each practice to garner input, and we incorporated their feedback. Perhaps due to this slow, methodical process, we encountered very little resistance, just appropriate questions and concerns from team members leading to productive conversations.
Partner with your organization. When our department was about one year into this QI project, our larger organization, Prisma Health, recognized the success of our approach and began to develop QI structures for the entire organization. They developed a new centralized BP data set, including leading metrics, and invested IT resources to create a simpler way for practices to view their metrics. The data is extracted from the EHR and housed on a separate platform but updated in real time, which allows rapid identification of performance improvements or lapses. Now, instead of having to use a laborious manual process, any team member can quickly review a site's rate of BP recheck, follow-up, and control. Our department's hypertension management algorithm was adapted slightly and approved for all primary care departments, and the medication advancement algorithm was integrated into our EHR for easier ordering. As a result, our QI efforts are impacting care at more than 60 offices. Assessment of system-wide interventions is currently underway.
RECOMMENDATIONS FOR APPLICATION
We encourage other primary care physicians to undertake similar QI projects in their practices. The key to getting your team engaged is to choose meaningful metrics, so remember the following:
- We are all more likely to engage in quality incentive programs if we are being assessed for something over which we have control. Find evidence-based, leading metrics within the power of your team to address, and focus on those.
- We are here for our patients, not the metrics, so choose metrics that are patient oriented. If you are proposing a change in workflow, documentation, or the standard of care, make sure it is abundantly clear why the change will be clinically better for the patient as an individual, not just as a number on a spreadsheet.
If you choose your metrics well, the end goal of improved care and saved lives will come with time.
