
These evidence-based strategies can help you understand your patients' context so you can better care for and empower them.

Primary care is a demanding field, requiring a high cognitive load due to complex patient histories, broad differential diagnoses, multiple treatment options, expanding medication lists, and a variety of team members. Physicians are tasked with managing all of these variables while also communicating well with patients to create a detailed picture of their health.
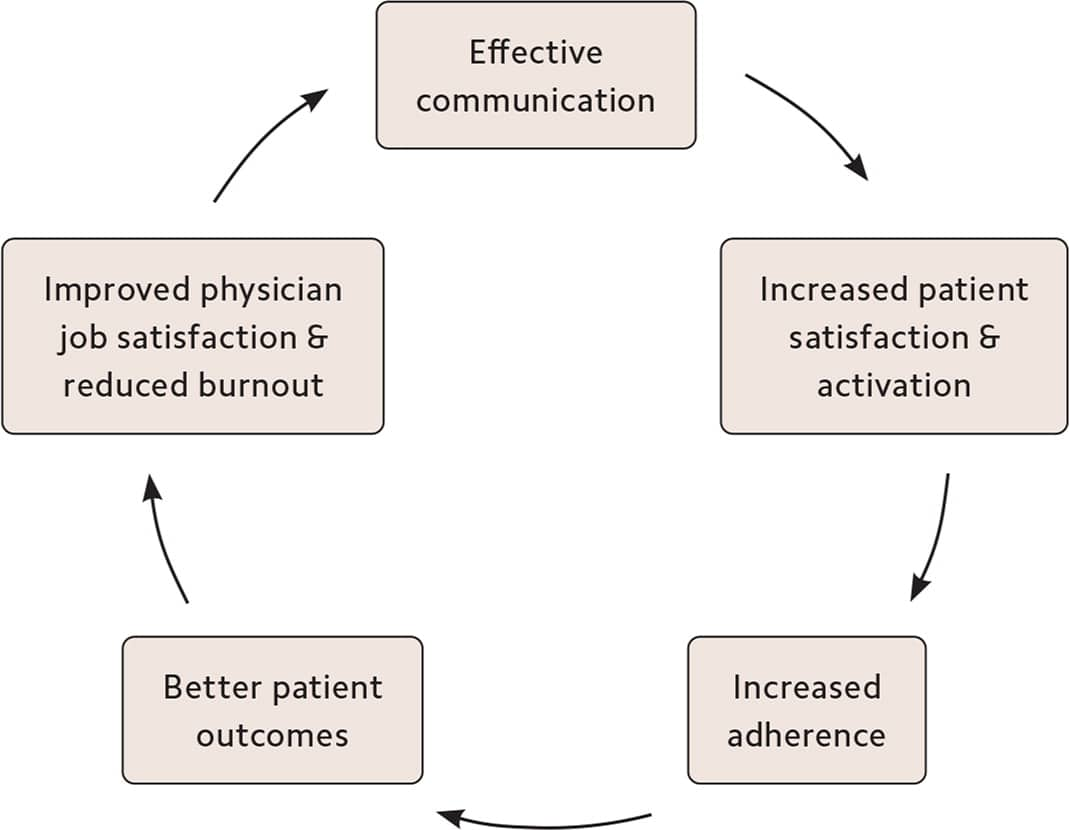
However, research has consistently found gaps in patient comprehension of even basic components of their visits,1 and patients often express that their physician does not fully understand their concerns or undervalues their perspective.2 Overcoming these barriers is crucial, as improved communication enhances not only the exchange of information but also the therapeutic relationship.3,4
THE IMPORTANCE OF EFFECTIVE COMMUNICATION
Effective communication often requires a trauma-informed mindset, given that roughly half of primary care patients have undergone some form of trauma.5 This means approaching each patient with empathy and curiosity about “What happened to you?” rather than “What is wrong with you?”
This article presents five communication strategies that can help create psychological safety, build trust, and facilitate better patient interactions, particularly with individuals who have experienced trauma.
KEY POINTS
- Clear and effective communication improves patient satisfaction, treatment adherence, and health outcomes.
- Effective communication often requires a trauma-informed mindset; this involves approaching patients with empathy and curiosity about their experiences and creating psychological safety.
- Evidence-based communication strategies include perspective-taking, emotional attunement, patient activation, shared decision-making, and teach-back.
PERSPECTIVE-TAKING
When patients enter the examination room, they bring with them their own unique background, including race, gender, profession, spirituality, fears, biases about the health care system, lived experiences, and their community's opinions. The simple practice of imagining yourself as the patient, looking at the situation through the patient's eyes, can increase patient satisfaction6 and help combat bias.7 It can also benefit physicians, protecting against burnout by reducing clinical monotony, increasing pro-social helping behaviors, and supporting their emotional balance.8
To use perspective-taking in a patient encounter, take a moment before you step into the exam room and imagine that you are the patient. Consider their potential experiences, biases, fears, and hopes. Perhaps they are feeling skeptical, tired, in pain, or overwhelmed while having to interact with a physician they may perceive as intimidating, naive, dismissive, or even adversarial. Enter with a sense of curiosity and flexibility, and invite the patient to help you understand their perspective.
Perspective-taking in action:
- “I can only begin to understand what you're going through. Please tell me more.”
- “What's your take on the situation?”
- “I think I get what you're saying. [Repeat it back.] What am I missing?”
EMOTIONAL ATTUNEMENT
A patient's emotions can sometimes seem to obscure the clinical picture, but in reality their emotions are an essential part of the picture. Being aware of and responsive to the patient's emotions, without being overcome by them, can enhance clinical decision-making because it clarifies aspects of the patient's experience that may be relevant to the diagnosis or treatment plan.9
To engage with patients in a way that honors their emotional state, think of yourself as an ally. If the patient is expressing an emotion such as fear or grief, imagine yourself standing shoulder to shoulder with the patient, encountering the source of fear or grief together. At times, you may need to use your connection with the patient to deescalate emotions and engage the patient in the task at hand, such as forming a treatment plan. But spending even a few moments attending to the patient's emotions will build trust, facilitate more honest communication, and forge a stronger therapeutic relationship.
Emotional attunement in action:
- “I appreciate you sharing your feelings with me; it helps me understand your perspective better.”
- “Goodness, you must be in a great deal of pain.”
- “Wow. This is such a difficult situation. How are you feeling?”
- “I am so sorry you're dealing with this. I will be with you through this process.”
PATIENT ACTIVATION
Patient activation is about helping patients understand the important role they play in their own health and then increasing their willingness and ability to participate in their care and maintain positive health behaviors over time.10 Studies have shown that a patient's engagement with and trust in their physician translates to greater patient activation,11 and primary care physicians who believe the patient role is important are more successful in promoting positive health behaviors.12
To improve patient activation, ask the patient for their ideas (e.g., how to reach a specific health care goal), personalize treatment options based on your knowledge of the patient, and consider increasing established communication (e.g., by using text reminders about the patient's health goals). Patients tend be more activated if they feel that a goal is achievable and they have the tools to make it happen. Although medical appointments are often focused on symptoms, problems, and deficits, be sure to also listen for and reinforce strengths that may help the patient feel more confident in their capacity to execute the plan. Ultimately, the patient is “captain of the ship,” and the physician is a trusted navigator and advisor.
Patient activation in action:
- “I'm here to provide the tools and knowledge you need to feel empowered in your health decisions. What would make you feel more confident in your ability to execute the plan we developed today?”
- “What have you learned from past experiences that could help you moving forward?”
- “What challenges do you foresee in making these changes, and how can I support you?”
- “Can you use the patient portal to message me or the care team when you have concerns?”
- “It's great that you're taking initiative. Let's explore how to make that easier for you.”
Shared decision-making is the process by which a patient and physician collaborate to build the best care plan, integrating the physician's medical knowledge with the patient's context and preferences. When health care decisions are truly collaborative, both parties feel more valued, patient outcomes improve,12 and patient satisfaction increases.13
The Agency for Healthcare Research and Quality's SHARE model begins with seeking the patient's participation.14 The physician then helps the patient understand and compare their options, assesses the patient's values and preferences, assists the patient in making an informed decision, and evaluates the decision, which includes monitoring the results and providing feedback and additional information.
Shared decision-making in action:
- “I want to make sure you feel confident about this decision.”
- “What would you like to discuss first?”
- “It sounds like you would prefer to try medication for a while before considering surgery. Do I have that right?”
- “I appreciate your input; it helps us create a treatment plan that aligns with your goals.”
- “What is most important to you when considering your treatment plan?”
- “Let's weigh the pros and cons together to find the approach that feels right for you.”
TEACH-BACK
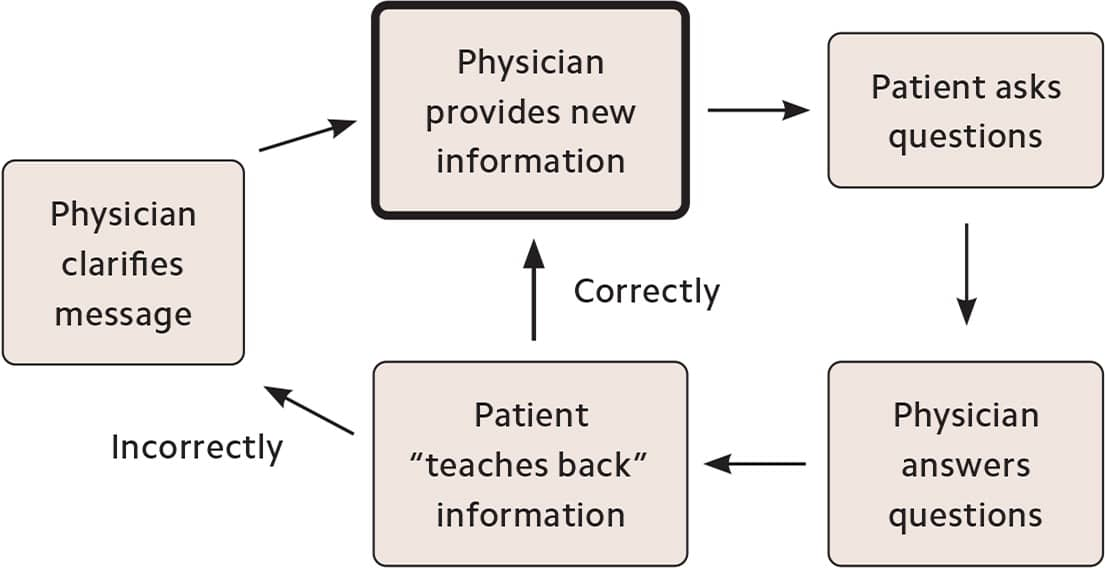
Teach-back is a strategy wherein the physician asks the patient to explain in their own words what was discussed during a visit, in order to assess how well the patient has understood the information. There are multiple reasons a patient may not comprehend a message. They could have an undiagnosed sensory deficit, a cognitive or language impairment, or poor health literacy. Or they could feel intimidated, overwhelmed, frightened, exhausted, or in pain. Whatever the reason, repeatedly assessing patient understanding is essential when transmitting important information and has been shown to have a positive impact on a range of outcomes, including treatment adherence and reduced hospital readmissions.15
The teach-back method begins with the physician explaining a concept to the patient (e.g., the risks of a medication) and then asking the patient to repeat back in their own words what the physician said. At that point, the physician can address any misunderstandings or gaps in knowledge or confirm the successful exchange of information.
THE TEACH-BACK METHOD
Teach-back in action:
- “Can you review your medications with me and why you should take them?”
- “What are the key points you'll remember from our conversation today?”
- “I want to make sure we're on the same page, so can you share what you understood?”
- “Can you share with me your plan until your next clinic visit?”
- “What did we just review about your current treatment plan?”
PUTTING IT INTO PRACTICE
The five trauma-informed strategies presented in this article can improve communication between physicians and patients, leading to more effective and satisfying interactions. But like any technique, they require some practice. To get started, pick one or two strategies, and try them with one patient this week.
Here's how that might look:
You are about to see Maria, a new patient in her late 40s who has been experiencing chronic pain for several months. Before entering the exam room, you take a moment to imagine the situation from Maria's perspective. In addition to being in pain, she might be feeling frustrated and worried that she doesn't yet have a clear diagnosis or treatment plan.
In the exam room, you greet Maria and say, “I can only begin to understand what you're going through. Please tell me more about your pain and how it's affecting your daily life.”
She describes that her pain is mostly in her lower back and abdomen and it has gradually increased over the past six months. She says she can't sleep well and it's hard to focus at work. “I feel like no one understands how much this pain is affecting me,” she says.
You respond, “I am so sorry you're dealing with this. Let's work together to find out what is causing your pain and how we might alleviate it.”
By employing two of the five communication strategies — perspective-taking and emotional attunement — you have set the stage for an open and trusting relationship, which will lead to greater patient activation and adherence, and ultimately better outcomes and satisfaction.
SUMMARY OF THE FIVE COMMUNICATION STRATEGIES AND SAMPLE PHRASES
Download a one-page summary of the five strategies and sample phrases to use with patients.
