
Conversations about safe driving can be more effective if you start early, consider functional dependence, and tailor recommendations to the patient's stage and type of dementia.

Primary care clinicians are often asked to assess older patients' fitness to drive but may feel underprepared for these assessments.1 When patients have a dementia diagnosis, the guidelines are seemingly straightforward: Those with moderate or severe dementia should no longer drive.2,3 But putting the guidelines into practice can still be challenging. For patients with mild cognitive impairment or early-stage dementia, the guidelines allow them to drive, but as many as one in three may still fail a behind-the-wheel driving test.4 Those patients may benefit most from in-depth assessment and counseling about their driving safety. In the later stages of dementia, patients are less likely to have insight into their driving ability and may not remember past conversations about driving cessation.
Navigating these complex conversations starts with gathering focused information about the patient's dementia stage, type, and impact on driving and then applying four key considerations when discussing driving safety.
KEY POINTS
- Start conversations about driving safety at the earliest signs of dementia to help ensure that patients, rather than their surrogates, are part of the decision-making process.
- Consider whether to refer a patient for a driving assessment, whether your state requires you to report concerns about a patient's driving ability, and whether your language is empathetic when speaking with patients about driving cessation.
- Compile resources ahead of time to help patients and their caregivers prepare for driving restrictions and the associated grief.
DETERMINING DEMENTIA STAGE, TYPE, AND IMPACT ON DRIVING
Physicians can quickly and effectively determine a patient's stage of dementia at each encounter by assessing functional independence and how this has changed over time. These determinations rely on the patient's ability to perform the following:
- Activities of daily living (ADLs), which include managing basic physical needs such as personal hygiene, toileting, eating, and dressing,
- Instrumental activities of daily living (IADLs), which require more advanced skills and support overall well-being such as managing finances, managing medications, preparing meals, and cleaning the home.
When asking about functional dependence, it's important to distinguish between changes due to cognitive impairment as opposed to other factors such as mood, personality, or a physical limitation. In general, if a patient has functional dependence in one or more ADLs due to cognitive impairment, they will also show functional dependence in their IADLs. A patient who is functionally dependent on others for at least one IADL has at least mild dementia, which warrants a conversation about driving safety. A patient who is functionally dependent on others for at least one ADL (often starting with difficulty choosing appropriate clothes or going through their personal hygiene steps when they bathe/shower) has at least moderate dementia, and guidelines state you should recommend they no longer drive.
A patient who is able to perform all IADLs and ADLs generally does not require a conversation about safe driving unless they exhibit other symptoms that suggest mild cognitive impairment and may impair driving, such as slower reaction time.
Explaining these stages to patients and their families is a worthwhile investment of time and may empower families to focus on function and safety in a structured way. Asking what new challenges patients with dementia are facing cognitively and functionally can help clinicians update how they might counsel patients about important tasks like driving.
Determining not only the stage but also the type of dementia the patient has can help clinicians tailor their driving recommendations. For example, the concerns for a patient with mild Alzheimer's include not only the risk of a crash but also the risk of “wandering” or getting lost while driving.5 These patients might be able to prolong their safe driving by only driving with a passenger (which positions family, friends, and care partners to observe changes in the patient's driving behavior earlier) or using GPS in the car to provide navigation. Patients with even mild Alzheimer's dementia can be at increased risk for tactical driving errors (e.g., difficulty yielding at intersections, changing lanes, or checking blind spots),5,6 so it is valuable to ask them and their passengers about this regularly.
Other types of dementia are associated with different and potentially more severe driving challenges. Even in the early stages of vascular dementia, for example, as many as 70% of patients fail on-road driving assessments.7 Patients with frontotemporal dementia are more likely to exhibit impulsivity and dangerous driving behavior. Patients with Lewy body dementia or Parkinson's disease dementia may experience motor disturbances and cognitive impairments in domains critical for driving (e.g., visual-spatial processing, executive function, and attention) in addition to tactical driving errors.
FOUR KEYS TO BETTER DISCUSSIONS
Conversations about safe driving can be more productive if clinicians keep the following points in mind.
1. Start early. It is better to talk with patients about driving safety before they progress to moderate or severe stages of dementia for several reasons. First, it increases the likelihood that they will be able to participate in shared decision making to plan for the transition to not driving, rather than requiring a surrogate to do so. Second, patients with early-stage dementia may already need to modify their driving behavior (e.g., only driving in familiar areas or during daylight hours) or even stop driving altogether. Even mild stages of dementia are associated with an increased likelihood that a patient will fail a driving test.8
Starting an ongoing conversation about driving safety with your patients at the first signs of dementia also allows you to use a “warning shot” approach.9 This lets patients know to expect future discussions about their driving safety before the conversation becomes a recommendation that they not drive — or worse yet, a report to driver's licensing authorities that the patient is a hazard to themselves or others behind the wheel (more on that in key No. 3). Many patients with mild dementia may be aware and accept that they will not be safe to drive independently in the future and may enter a period of “worried waiting.”10 Starting conversations about driving safety with them early can give them time to plan for their driving retirement, as well as a sense of agency about the decision. This is better than waiting for a crisis, such as a crash, to trigger an abrupt transition to driving cessation.11
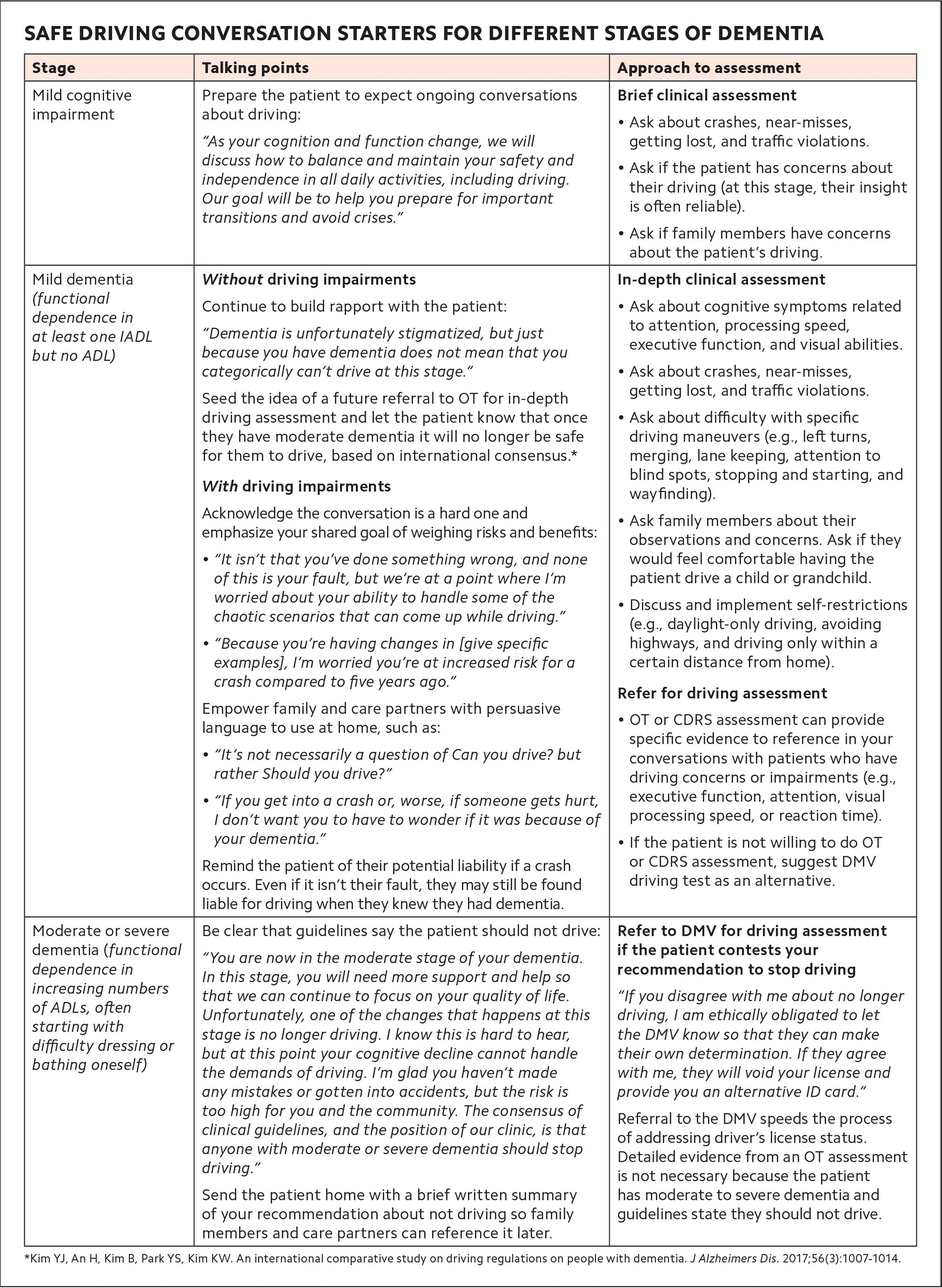
Indeed, some patients may welcome these conversations and even initiate them. But for most patients, talking about giving up driving is difficult, particularly if they see the transition as a significant loss of independence. Patients may be reluctant to raise concerns, and their partners might worry about “tattling” on them. Therefore, clinicians often have to invite and initiate conversations about driving. (See “Safe driving conversation starters for different stages of dementia.")
2. Understand options for driving assessments. There are a wide range of tests for determining a patient's fitness to drive — most of which are not well-suited to the time constraints of a primary care setting. Once you determine a patient's stage and type of dementia, it can be useful to refer patients with mild dementia whose driving ability is questionable to an occupational therapist (OT) or a Certified Driver Rehabilitation Specialist (CDRS) — often an OT with specialized training.
Depending on the practice setting, OT assessments may involve cognitive tests or driving simulations. They don't necessarily include behind-the-wheel testing, which can be a source of frustration for patients who want a professional to evaluate their competence in real-world driving scenarios, so it's best to prepare them for this before you make the referral. A CDRS is more likely to provide a behind-the-wheel evaluation as well as vehicle modifications and training to extend safe driving if possible, but these specialized services may not be covered by patients' insurance. Clinicians and patients can find driving rehabilitation services in their area using the American Occupational Therapy Association's search tool.
3. Know your state's reporting requirements. If state law requires you to report concerns about a patient's driving ability to driver's licensing authorities or refer them to licensing authorities for a driving assessment, you may want to explain that to your patient. Regulations vary by state, so check with your lawyer, department of motor vehicles (DMV), or similar entity. Reporting requirements may also influence the potential for you to be found liable for injuries or damages if your patient is in a crash. In general, a clinician is most at risk of being found liable in cases when the patient might reasonably have been unaware of how a treatment (e.g., medication) or condition (e.g., dementia) might endanger their driving ability because their clinician failed to warn them. Therefore, you should document any discussions you have with patients about driving safety.
Depending on your state's policies, you may also be able to recommend restrictions for a patient's license. For example, in Wisconsin, clinicians are not required to report driving concerns to the DMV, but they are encouraged to do so and can recommend certain enforceable restrictions such as daylight-only driving, driving only within a five-mile radius of the patient's home, driving only within the city limits, continuous oxygen use while driving, or no freeway/interstate highway driving.
4. Use empathetic language. The discussion of safe driving may feel premature to some patients with cognitive impairment or dementia, particularly if they have not had any significant accidents behind the wheel. It is important to be sensitive to their feelings and not minimize the downsides of being unable to drive. People who stop driving are at risk for multiple adverse health outcomes, including increased depression and social isolation.12 Many older adults describe feelings of grief caused by the loss of independence and enjoyment they get from driving.10,13 Being up front about this shows that you understand the gravity of the conversation and you're not taking it lightly. This is a major life change, and to best support patients, you can approach conversations about driving cessation as you would other “bad news” that brings major life changes (e.g., diagnosing a chronic condition or a progressive illness). It's vital to acknowledge the emotional challenges and connect patients to resources (see “Resources for patients and families”) that can help them prepare — emotionally and logistically — to stop driving. Your state DMV may also have resources.
RESOURCES FOR PATIENTS AND FAMILIES
- Plan for the Road Ahead (East Carolina University)
- Family Conversations With Older Drivers (The Hartford)
- Dementia and Driving (Alzheimer's Association)
IDEAS FOR PUTTING IT INTO PRACTICE
Evaluating driving risk in patients with dementia can take different forms in a busy clinical practice.14 When pre-charting before seeing a patient with dementia, determine whether a conversation about driving safety should occur and, if so, whether a referral for driving evaluation or mobility planning may be necessary. Provide resources to the patient via an EHR smart-phrase or handout to maximize time spent talking with the patient and family. Work within your clinic or health system to develop a shared resource list and assign stakeholders to keep it updated. Discuss driving cessation empathetically and regularly with the patient over time. Ultimately, this can normalize the conversation, highlight its importance, and lead to better outcomes for the patient and the community.
