Senile dementia of the Binswanger's type is a term used to describe a dementia syndrome characterized by onset in the sixth or seventh decade of life, subcortical neurologic deficits, psychiatric disorders and evidence of hypertension or systemic vascular disease. The status of senile dementia of the Binswanger's type as a distinct entity is a matter of some controversy. The array of neuroimaging abnormalities and clinical findings attributed to this condition overlap with a number of other neuropathologies. Leukoaraiosis, or attenuation of subcortical white matter, seen on computed tomographic scans or magnetic resonance imaging of the brain, is a hallmark of senile dementia of the Binswanger's type. The clinical findings associated with Binswanger's disease are varied but typically include a progressive dementia, depression and “subcortical” dysfunction such as gait abnormalities, rigidity and neurogenic bladder. Treatment is largely supportive and includes a discussion about advanced directives, social support and antidepressant therapy. Control of hypertension and aspirin prophylaxis may help prevent further progression of white matter disease.
Senile dementia of the Binswanger's type, or Binswanger's disease, was once believed to be a rare form of dementia. As neuroimaging modalities such as computed tomography (CT) and magnetic resonance imaging (MRI) have become more commonly available, the idea that senile dementia of the Binswanger's type is a more common form of dementia and neurologic disease has become more widespread.
Numerous names have been given to this condition (Table 1). In 1894, Binswanger first described a form of dementia called encephalitis subcorticalis chronica progressiva, separate from neurosyphilis and other forms of dementia in the elderly. He characterized the disease as being associated with lesions of the subcortical white matter with “severe atheromatosis of the arteries,” enlarged ventricles and normal cortex. The term “Binswanger's disease” was first used in 1902 by Alzheimer to identify this form of senile dementia. The term “subcortical arteriosclerotic encephalopathy” was first used in 1962, and the term “multi-infarct dementia” began to be used in 1974.1,2 Multi-infarct dementia is a broader term for vascular dementia and includes both Binswanger's dementia and the dementia resulting from repeated thrombotic and embolic cerebral infarcts. The term “senile dementia of the Binswanger's type” was recommended in 1987.3
TABLE 1 Other Terms for Senile Dementia of the Binswanger's Type
| Binswanger's dementia |
| Binswanger's disease |
| Binswanger's encephalopathy |
| Subcortical ischemic disease |
| Subcortical ischemic leukoencephalopathy |
| Subcortical arteriosclerotic encephalopathy |
| Progressive subcortical vascular encephalopathy |
| Encephalitis subcorticalis chronica progressiva |
| Lacunar dementia |
It is still a matter of some controversy whether senile dementia of the Binswanger's type constitutes a distinct clinical entity4,5 or is simply descriptive of the shared end result of a number of diverse neuropathologies that affect subcortical white matter. As computed tomography (CT) and magnetic resonance imaging (MRI) of the brain become more common in the elderly, family physicians often encounter patients with brain abnormalities that are labeled Binswanger's-type lesions. This article reviews both the clinical and the neuroradiologic features that are most commonly attributed to senile dementia of the Binswanger's type.
Dementia
Dementia is defined as a syndrome of multiple acquired cognitive defects occurring without acute confusion (delirium). All cases of dementia deserve careful evaluation for the possibility of reversible causes, such as hypothyroidism or vitamin B12 deficiency. Vascular dementia is recognized as a common form of dementia, second to Alzheimer's dementia. The third leading cause of dementing illness is a combination of Alzheimer's dementia and vascular dementia. This combination may be difficult to diagnose.
Several types of vascular dementia result from various forms of brain injury. Mechanisms contributing to these dementias include lacunar stroke, cardiogenic emboli and atherothrombotic emboli. A single cortical infarct that occurs in a certain position can result in unique features that indicate the specific region of the brain that is affected. This type of injury will not typically result in defects of multiple cognitive domains, as occur in dementia. Multiple cortical infarctions, however, can result in a “patchy” pattern of cognitive deficits.
Subcortical lesions can also lead to dementia. Senile dementia of the Binswanger's type describes a form of subcortical vascular dementia with certain lesions of the white matter and specific clinical features.
Illustrative Case
A 57-year-old man who was a nonsmoker was brought to the family physician's office by his wife. The patient's chief complaint was malaise. His wife reported that the patient had hypersomnia, poor memory and concentration, social withdrawal and a lack of interest in his usual activities. The patient had a past history of hypertension and heavy ethanol use. He denied having morbid thoughts, recent stressors or suicidal ideation. On examination, his blood pressure was 160/98 mm Hg; he had a flat affect and a depressed mood. The patient was alert, oriented and appropriate, with marked psychomotor retardation, a paucity of communication and no evidence of thought disorder. The patient's deep tendon reflexes were slowed, and the rest of the physical examination was normal.
The patient appeared to be severely depressed and was prescribed fluoxetine. Improvement was minimal despite an increase in the dosage of antidepressant. Results from a fasting blood profile, thyroid function tests, vitamin B12 measurement, syphilis serology, cortisol measurement and complete blood cell count were unremarkable. A CT scan revealed mild cerebral atrophy and no other findings. An electroencephalogram was normal.
The patient's employer reported that the patient had undergone an abrupt personality change. His personality had changed from jovial with a good sense of humor to docile, introverted and unwilling to confront typical work situations. His work performance deteriorated. He slept during important meetings and was frequently found wandering among the buildings. Mistakes were hidden by his fellow employees.
MRI scanning of the brain demonstrated multiple focal areas of increased T2-weighted signal in the periventricular region, right and left cerebellar hemispheres and basal ganglia (Figure 1). Neuropsychiatric testing revealed cognitive impairment; a psychiatry consultation suggested an organic mood disorder; a neurologic consultation confirmed the suspicion of dementia caused by Binswanger's disease. The patient's mental condition continued to deteriorate and a year later, a cerebrovascular accident left the patient with mild left hemiparesis. Nursing home care was subsequently required.
FIGURE 1.
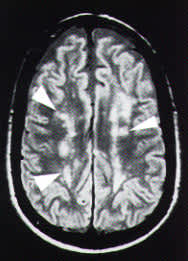
Magnetic resonance image of the brain, T2 axial view without contrast enhancement, of the patient in the illustrative case. Note the areas of increased signal bilaterally, known as periventricular hyperintensity (arrows).
Pathophysiology
The age of onset of senile dementia of the Binswanger's type is typically in the sixth and seventh decades of life, and men and women appear to be affected equally often. The incidence of the disease is difficult to cite given the controversies regarding its clinical features but has been reported to range from 3 to 12 percent in the elderly.6
The exact etiology of senile dementia of the Binswanger's type is unclear, although theories concerning alterations in vascular permeability and the blood-brain barrier exist. Diabetes, cardiac disease, previous cerebrovascular accident, malnutrition and, most notably, hypertension have been associated with senile dementia of the Binswanger's type.7,8 One study revealed that 75 percent of patients with characteristic CT findings of senile dementia of the Binswanger's type on CT scan had hypertension, 60 percent had a history of acute stroke or transient ischemic attack and 50 percent had other forms of vascular disease.8 Some rare, perplexing cases without the features of hypertensive or vascular disease have also been reported.9 Other proposed risk factors for senile dementia of the Binswanger's type include small artery disease such as arrhythmias, amyloid angiopathy, impaired autoregulation of cerebral blood flow, and periventricular hypoperfusion resulting from cardiac failure. Conditions affecting blood viscosity, such as antiphospholipid antibody syndrome, neoplasms, polycythemia and severe hyperlipidemia, have also been associated with senile dementia of the Binswanger's type.4
The gross pathology of brain tissue from patients with senile dementia of the Binswanger's type reveals gyral atrophy and sulcal widening, resulting from loss of supporting cerebral white matter. Lacunar infarctions are seen in the white matter, pons and basal ganglia in over 90 percent of cases and, on occasion, in the cerebellum. Lateral ventricular enlargement is found in over 95 percent of cases. Atheromatous changes of the large cranial vessel are present in 93 percent of cases.10
The histopathology of senile dementia of the Binswanger's type is marked by diffuse and patchy loss of myelin in the cerebral white matter, with areas of reactive gliosis. Nerve fibers are decreased.11 The small penetrating arteries of the deep white matter show fibrous thickening compatible with hypertensive disease.
The periventricular white matter of the brain is a so-called watershed area, with a blood supply that is particularly vulnerable to hypoperfusion. An elevated plasma viscosity enhancing this hypoperfusion also may play a role in Binswanger's disease.12 Microscopic infarcts or lacunae and edema are also found, although vessel occlusion is rare. The cerebral cortex itself often appears normal or with only minimal findings. The histologic severity of senile dementia of the Binswanger's type correlates with the degree of findings on neuroimaging.13 Other autopsy findings commonly demonstrate systemic evidence of longstanding hypertensive disease.
Neuroimaging
Characteristic CT changes of senile dementia of the Binswanger's type include areas of noncontrasting hypodensities that are nearly symmetric in the periventricular white matter. This hypodensity is often called “leukoaraiosis.” Complicating the specific diagnosis of Binswanger's disease is the fact that leukoaraiosis is commonly found in symptomatic elderly patients5 and in up to 100 percent of patients with Alzheimer's dementia in some studies.4 Some authors have suggested that specific patterns of leukoaraiosis are more common in patients with senile dementia of the Binswanger's type, but this suggestion is not universally accepted. MRI is much more sensitive than CT in visualizing these white matter lesions, which appear as areas of periventricular hyperintensity on T2-weighted images. Unfortunately, this increased sensitivity is complicated by a much lower specificity, since a number of other neuropathologies display similar white matter lesions (Table 2).
TABLE 2 Periventricular White Hyperintensities on MRI: Differential Diagnosis
| Multiple sclerosis |
| Progressive multifocal leukoencephalopathy |
| Acute disseminated encephalomyelitis |
| Postradiation effect |
| Leukodystrophies |
| Perilesional edema from tumor or stroke |
| Encephalitis of AIDS |
| Normal pressure hydrocephalus |
MRI = magnetic resonance imaging; AIDS = acquired immunodeficiency syndrome.
The pattern of periventricular hyperintensity seen on MRI in patients with senile dementia of the Binswanger's type is typically intense, with variable thickness, patchy distribution and irregular margins. Lacunae are often apparent in the basal ganglia and thalamus. Ventricular enlargement is found in most patients with Binswanger's disease. This hydrocephalus is believed to be due to volume loss of periventricular white matter and cerebrospinal fluid absorption into the surrounding tissue.3 This finding may be confused with the diagnosis of normal pressure hydrocephalus, which may also exhibit periventricular hyperintensity. However, in cases of normal pressure hydrocephalus, areas of hyperintensity are typically smooth and symmetric, and fail to extend dorsally, unlike those in senile dementia of the Binswanger's type.14
Single-photon emission computed tomography (SPECT) is expensive and usually available only in larger urban areas. SPECT scanning may be useful when the diagnosis of dementia of Alzheimer's type is in question. Characteristic metabolic patterns that are apparent on SPECT can help differentiate dementias in cases that are not clear.
The characteristic CT or MRI findings of Binswanger's disease carry many other diagnostic possibilities and require careful clinical correlation3,15,16 (Table 2). Neuroimaging alone is too nonspecific to establish the diagnosis of senile dementia of the Binswanger's type. All patients with dementia require a thorough evaluation to rule out metabolic and reversible forms of dementia.
Clinical Features
A wide array of clinical features have been attributed to senile dementia of the Binswanger's type by a number of authors, leading to some controversy.4,5,10 To be more specific in the diagnosis of senile dementia of the Binswanger's type, most authors agree that the diagnosis should not be based on neuroimaging findings alone but on those findings in combination with clinical findings. Table 3 lists proposed criteria for diagnosing senile dementia of the Binswanger's type.17
Course of the Disease
In one third of patients, the onset of the disease is sudden, with acute neurologic deficits consistent with a diagnosis of stroke. Two thirds of cases begin slowly and insidiously. Focal neurologic findings may or may not be present. The subsequent course of the disease varies, with gradual progression or stepwise deterioration. In a few cases, periodic improvement and stability have been reported.
The gradual progression of memory loss is the most commonly reported symptom; it may be less profound than that in patients with Alzheimer's dementia.18 Mental status changes are the predominant feature. Apathy, a loss of interest in usual activities, depression, confusion, paranoia and personality changes are frequently noted. Disorientation, dependence on others and difficulties in judgment present later in the course of Binswanger's disease.
Signs
Most patients with senile dementia of the Binswanger's type demonstrate a variety of neurologic findings. Mild asymmetric pyramidal signs (reflex asymmetries, hemiparesis), extrapyramidal signs (rigidity) and cerebellar signs (limb and gait ataxia) are the most common findings.19 Frequent falls and syncopal episodes are an early sign of Binswanger's disease, and hypoperfusion of the brain has been suggested as a cause.20 Gait disturbances are present in over one half of cases. Using the legs to walk is more difficult than using the lower extremities in other motor tasks while lying or sitting. In contrast, facial and upper extremity function is fairly well preserved.21 Pseudobulbar palsy may be present (dysarthria, dysphagia, labile laughing or crying). Mutism and parkinsonism are common in advanced cases.19 Incontinence and seizures may also occur in more advanced cases.22
Psychiatric Findings
Affective disorders are a prominent feature of senile dementia of the Binswanger's type. Before the diagnosis is confirmed, the psychiatric findings in Binswanger's disease are frequently confused with those of other mental illnesses. These mental status changes are typically found early in the course of the disease and may not accompany the neurologic findings. The changes vary in onset and severity but are present in most cases.
Alterations in mood and behavior are a predominant feature of senile dementia of the Binswanger's type. Patients may become emotionally labile and unpredictable, demonstrating euphoria or aggression. Severe depression occurs in 20 percent of cases, and suicide attempts have been reported. Delusional behavior, paranoia and psychosis may occur.23
Treatment
No treatment is known to reverse or cure senile dementia of the Binswanger's type. There are implications that control of hypertension may slow progression of the disease and aspirin therapy may prevent future cerebral infarcts. No studies substantiate the outcome of these preventive measures, although treatment of high blood pressure and the appropriate use of aspirin prophylaxis are generally instituted.
Therapies that target blood hyperviscosity, a potential contributing factor in all brain angiopathies, are under investigation.4 Caplan4 recommends smoking cessation, with phlebotomy in patients with a hematocrit greater than 45 percent.
As with any progressive dementing illness, support must be given to both the patient and the caregivers. The family physician should evaluate the patient's social supports, resources and needs. A discussion of advanced directives, such as living wills and resuscitation orders, is appropriate. The treatment of concurrent medical problems such as diabetes and cardiac disease is important and beneficial to the patient's overall well-being. Emphasis on function, through maintaining mobility and using cues and reassurance for memory disruption, is essential.
Support groups and organizations may be helpful to families dealing with the emotional stress of caring for a demented relative. Supportive psychotherapy for caregivers may be indicated. The organic mood disorder of this condition can be distressing to both the patient and the family.
The depression associated with Binswanger's disease may be improved with antidepressant therapy.24 Since most patients are elderly, they are at risk for the typical side effects of antidepressants, such as hypotension or sedation. Although a selective serotonin reuptake inhibitor (SSRI) did not help the patient in the illustrative case, SSRIs, bupropion (Wellbutrin) or nortriptyline (Pamelor) may be tried. SSRIs are good choices for therapy in this age group because of their lower side effect profile, but studies of the efficacy of these antidepressants in patients with senile dementia of the Binswanger's type are limited. Lithium and monoamine oxidase inhibitors have been used successfully in some cases of senile dementia of the Binswanger's type.24,25
Final Comment
Senile dementia of the Binswanger's type is becoming more commonly diagnosed with the widespread use of CT and MRI brain imaging. While controversy still exists regarding its status as a distinct clinical entity, family physicians should be aware of the clinical and neuroimaging findings most commonly attributed to senile dementia of the Binswanger's type. The family physician can help educate the patient and family about this complex neuropsychiatric disorder and assist in a comprehensive care plan. A multidisciplinary approach with medical specialists such as a neurologist and psychiatrist, and ancillary personnel such as home health care nurses, mental health workers and social workers, is beneficial.
