A 21-year-old man presented with a soft, mobile mass 2 cm in diameter over the right lateral brow. The mass had been present since birth and had increased in size by approximately 20 percent in the past year. The patient denied having pain or visual disturbances. His medical and surgical histories were unremarkable. Neurologic examination revealed no abnormalities of the facial nerve or ocular motility and an absence of proptosis. Local excision of a presumed lipoma or epidermal inclusion cyst was attempted. Intraoperatively, an extensive cystic mass with a yellow, oily debris was encountered, and the mass extended into the temporal fossa. Incisional biopsy was performed and results of computed tomography showed the presence of a 3-cm × 2-cm mass in the subcutaneous and deep soft tissues lateral to the right orbit. Erosion into the temporal, sphenoid, and zygomatic bones was evident with no intracranial communication (Figures 1 and 2).
Figure 1.

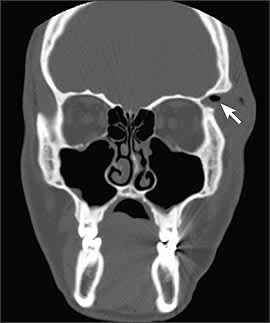
Figure 2.
Question
Based on the patient’s history, physical examination, and radiography results, which one of the following is the correct diagnosis?
A. Lipoma.
B. Teratoma.
C. Epidermal inclusion cyst.
D. Pilar cyst.
E. Dermoid cyst.
Discussion
The answer is E: dermoid cyst. Dermoid cysts are congenital abnormalities that result from the ectoderm failing to separate in the neural tube. The ectoderm can become trapped in a bony suture line during development, producing a bony abnormality. Over time, the cystic lesion grows and the patient may become symptomatic.1,2
The yellow, oily debris found on incision is typical of a dermoid cyst, and biopsy confirmed the diagnosis. The cyst lining consists of stratified squamous epithelium. The cyst is filled with debris, which is made from the products of the adnexal structures, such as sebaceous glands and hair follicles.1
The differential diagnosis for a dermoid cyst is extensive (see accompanying table).1–5 Often the diagnosis is not confirmed until histologic examination of the specimen is performed after biopsy. Dermoid cysts may be more involved than apparent on physical examination, as is true for many soft tissue tumors. Therefore, radiologic evaluation should be considered before excision in situations in which the margins are uncertain or the mass is located in a delicate area such as the face.
Selected Differential Diagnosis of a Chronic Soft Tissue Mass of the Head and Neck
| Condition | Characteristics |
|---|---|
| Bone cyst | Generic diagnosis for many types of bone cysts; may be slow growing or rapidly expanding; may expand intracranially; benign or malignant; asymptomatic or may present with symptoms such as headache |
| Branchial cleft cyst | Painful swelling; usually inferior to mandible on neck; slowly expanding; congenital |
| Dermoid cyst | Cystic mass with yellow, oily debris; slowly expanding; may extend intracranially; congenital |
| Eosinophilic granuloma | Localized pain, tenderness, swelling; most often involves skull or mandible; usually regresses spontaneously over one to two years |
| Epidermal inclusion cyst | Lateral in location; slowly expanding |
| Facial nerve neuroma | Painful, enlarging mass; neurologic impairment secondary to nerve palsy |
| Hemangioma | Erythematous macular patch or telangiectatic area with surrounding halo effect; most common benign tumor of infancy |
| Lipoma | Soft, mobile mass; may have multiple lesions |
| Liposarcoma | Slow growing, painless mass; may cause dysphagia and airway symptoms if pharynx involved; most are asymptomatic at presentation |
| Pilar cyst (wen) | Cystic mass filled with amorphous, keratinous material; located on scalp |
| Rhabdomyoma | Round, painless mass involving striated muscles of head or neck; benign |
| Rhabdomyosarcoma | Localized mass or swelling; may have cranial nerve involvement; location-dependent symptoms (e.g., nasal discharge, proptosis) |
| Teratoma | Midline, firm, painless; benign or malignant; congenital |
Lipomas are common, benign fatty-tissue tumors that often present in the same manner as dermoid cysts. If necessary, radiologic appearance may facilitate diagnosis; however, only histology will confirm the diagnosis.2
Teratomas are related embryologically to dermoid cysts in that they both arise from layers of the neural tube. In contrast to dermoid cysts, teratomas include all three germ cell layers: ectoderm, mesoderm, and endoderm. Seventy-five percent are considered mature teratomas and are benign. Teratomas usually present as a midline, firm, painless mass.3
Epidermal inclusion cysts are similar to dermoid cysts in that they are composed of stratified squamous epithelial cells but lack the adnexal structures. A laminated keratinous material fills the cyst. They typically are lateral in location and expand slowly.2
A pilar cyst (wen) occurs on the scalp as a freely mobile cystic mass filled with layers of keratinous material. However, the keratin produced by the epithelial lining is different from that produced by epidermal cysts. Cyst expansion disrupts hair growth, leading to alopecia over the lesion.5
