To the Editor: We report a case of an infant born at 38 and 5/7 weeks in compound presentation, via prolonged vacuum-assisted vaginal delivery, with a right, acute, nondisplaced Salter-Harris fracture involving the distal radial metaphysis. In the hours after delivery, the infant had right wrist swelling and bruising. The infant cried and became fussy when the arm was moved. Radiography showed a Salter-Harris fracture of the radius (Figure 1). Complicated vaginal deliveries can result in neonatal fractures, but Salter-Harris fractures resulting from vaginal delivery are rare. Early recognition and appropriate interventions can improve neonatal outcomes.
FIGURE 1.
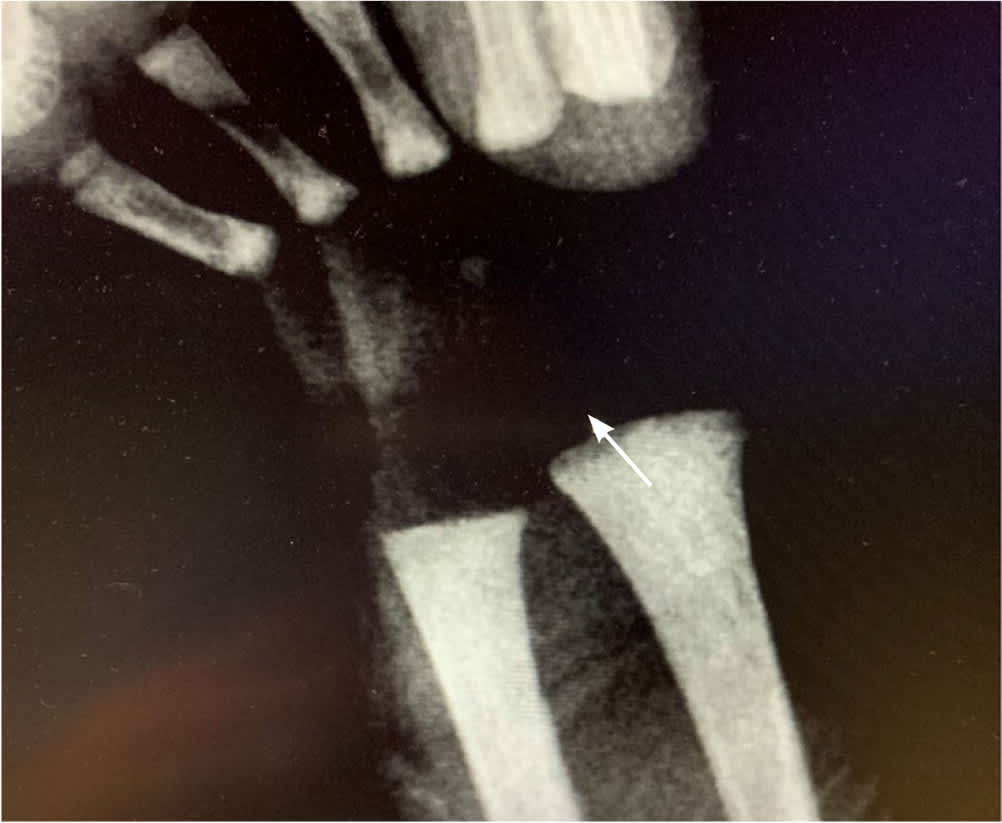
Salter-Harris fracture of the right radius in an infant.
Compound presentations involving a hand or foot complicate 1 in 300 to 1,300 deliveries.1 Certain pregnancy complications (e.g., fetopelvic disproportion, polyhydramnios, premature rupture of membranes) can increase the risk of compound presentations.1 A compound presentation is typically diagnosed during a vaginal examination where the presenting appendage can be palpated. The compound presentation may resolve on its own during labor; however, if not resolved, interventions such as manual reduction can be attempted. An operative delivery may be needed if a manual reduction is not successful.2
Fractures involving the growth plate can usually be treated conservatively with splinting.3 Orthopedics evaluated the infant three weeks later and found that healing was complete, with no continued splint or casting required. Salter-Harris type I fractures of the distal radius occur when force is applied through the physis, which splits the epiphysis from the metaphysis.4 A physical injury cannot be excluded if a patient is symptomatic. The radiographs may appear unremarkable because of a lack of bony involvement. Diagnosis is often based on clinical findings such as swelling and tenderness around the growth plate, which were seen in this infant.4
