Hearing loss is a prevalent, chronic condition in the United States; it is often gradual and progressive and is underreported by patients and undertreated by physicians. The impaired ability to effectively hear and communicate may result in negative emotional, cognitive, economic, and social consequences for individuals and may pose a safety risk. Questionnaires and smartphone apps are available to help identify and evaluate self-perceived hearing loss. Physicians should assess for objective hearing impairment when the patient or family member raises a concern or if cognitive or mood symptoms are present that could be influenced by hearing loss. Three types of hearing loss exist: conductive, sensorineural, and mixed. Pure-tone audiometry uses an audiometer and is reported on an audiogram; it is the most accurate method for hearing loss detection. It can be used for screening or comprehensive testing when combined with tympanometry, speech-reception thresholds, and word-recognition testing. Audiograms that show a unilateral or asymmetrical sensorineural hearing loss can be signs of retrocochlear pathology and warrant additional evaluation by an audiologist and otolaryngologist as well as imaging studies. Medicare Parts A and B do not pay for hearing aids, although some Medicare Advantage (Part C) or supplemental plans may provide insurance coverage for hearing aids. Less expensive, over-the-counter hearing aids may help mild to moderate hearing loss. Family physicians should counsel patients on the importance of protecting their hearing.
Hearing loss is one of the most prevalent chronic conditions in the United States, and it affects approximately 16% of the U.S. adult population.1 Consistent use of face masks during the COVID-19 pandemic sometimes revealed undiagnosed hearing loss, and patients with known hearing loss, especially those who are lip readers, experienced daily difficulties in understanding speech.2 Hearing loss is often gradual and progressive and is underreported by patients and undertreated by physicians.1,3 Untreated hearing loss has been associated with poorer objective physical functioning in older adults, increased risk for disability, and poorer quality of life.3 Hearing loss may result in negative emotional, cognitive, economic, and social consequences for individuals and may pose a safety risk.3–5
SORT: KEY RECOMMENDATIONS FOR PRACTICE
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to https://www.aafp.org/afpsort.
The U.S. Preventive Services Task Force concludes that there is insufficient evidence to assess the balance of benefits and harms of screening for hearing loss in adults 50 years or older.6 Some data endorse potential benefit in testing for adults with or without symptoms; the World Health Organization suggests screening adults 50 years and older every 5 years until 65 years of age, every 1 to 3 years in those older than 65 years, and whenever hearing loss is suspected.7–10
Risk factors for hearing loss include noise exposure, certain medications, tobacco use, and certain health conditions (e.g., autoimmune or cardiovascular disease, diabetes mellitus)11 (Table 112–15 ). More than 50% of patients with concerns of dizziness and imbalance, including falls, are seen by family physicians.16 Patients who have vestibular disorders are more likely to experience hearing loss than those without.11
TABLE 1. Risk Factors for Hearing Loss
| Condition | Examples |
|---|---|
| Chronic health conditions12,13 | Autoimmune disease (idiopathic or part of an established autoimmune condition), cardiovascular disease, diabetes mellitus, kidney disease, tobacco use disorder |
| Disorders of the ear12,13 | History of ear infections, labyrinthitis, Meniere disease, otosclerosis, vestibular schwannoma |
| Head or neck trauma, traumatic brain injury12 | Current or past injury or trauma, including blast or military combat injuries, falls, motor vehicle collisions, sports-related injuries |
| Noise exposure (occupational or recreational)13,14 | Acute exposure to impulse noise (> 130 decibels), chronic exposure over time (> 85 decibels), tinnitus |
| Ototoxic substances* 13–15 | Chemical exposure Asphyxiants (e.g., carbon monoxide, tobacco smoke) Metals (e.g., lead, mercury compounds) Nitriles (e.g., acrylonitrile, 3-Butenenitrile) Solvents (e.g., p-Xylene, styrene) Pharmaceuticals Aminoglycosides, other antibiotics (e.g., erythromycin†, gentamicin, streptomycin) Analgesics† and antipyretics† (e.g., acetaminophen, salicylates) Antineoplastic agents (e.g., carboplatin, cisplatin) Loop diuretics† (e.g., furosemide) Others† (chloroquine, hydrocodone, misoprostol) |
| Presbycusis12 | Increasing age, genetics |
| Other12 | Cerebellopontine angle tumors or neoplasms, stroke |
*—Commonly administered for hospital inpatients; patients who have pain, heart failure, chronic kidney disease; patients receiving chemotherapy.
†—Ototoxicity at therapeutic doses is limited and is typically reversible by decreasing or stopping medication.
Physicians should assess for objective hearing impairment whenever a patient or a family member raises a concern or if behavioral symptoms (e.g., decreased cognition, depressed mood) are present that could be influenced by hearing loss.12,17 Sudden unilateral hearing loss can be a medical emergency requiring urgent evaluation with audiometry. If sensorineural loss is identified, referral to an otolaryngologist within 2 weeks of diagnosis is recommended.12,18
Testing
The Hearing Handicap Inventory for the Elderly and the Self-Assessment of Communication questionnaires are suggested by the American Speech-Language-Hearing Association to help identify and evaluate self-perceived hearing loss.13,19,20 The AARP website has a hearing test available over the phone for a small fee; the test is based on the National Hearing Test, which is funded by the National Institutes of Health.21 Patients may also self-screen for hearing loss using an app on their smart phone.22 A systematic review found that uHear, Digits-in-Noise Test, HearTest, and HearScreen smartphone apps had sensitivities and specificities between 75% and 100%, which are accurate enough for use in screening23 (Table 224–27 ). Any abnormal findings on screening tests should be followed by formal testing or evaluation by an otolaryngologist. Special considerations should be incorporated during the evaluation to perform in-office audiometry correctly 12 (Table 328–38 ). As a result, fewer family physicians are performing in-office audiometry.
TABLE 2. Accuracy of Screening Tests for Moderate Hearing Loss
| Screening tests24 | Description of test | Hearing threshold | Sensitivity (95% CI) | Specificity (95% CI) | Positive likelihood ratio (95% CI) | Negative likelihood ratio (95% CI) |
|---|---|---|---|---|---|---|
| Finger rub (one study, n = 107) | Rubbing fingers together 6 inches from ear Positive test: failure to hear the rub in at least three of six attempts | > 40 dB | 35 (26 to 46) | 97 (90 to 99) | 11.67 (NR) | 0.67 (NR) |
| Hearing Handicap Inventory for the Elderly (five studies; n = 2,820; pooled data) | 10 questions on social and emotional handicap because of hearing loss Positive test: score higher than 8 | > 35 to 40 dB | 68 (52 to 81) | 79 (64 to 84) | 3.21 (2.4 to 4.2) | 0.41 (0.28 to 0.59) |
| Pure-tone audiometer screener (four studies, n = 411) | Device emits a pure tone and patient states whether they can hear it Positive test: inability to hear 40 dB at 500, 1,000, or 2,000 hertz in one or both ears | > 35 to 40 dB | 94 to 100 (NR) | 24 to 80 (NR) | 9.2 to 15.6 (NR) | 0.06 to 0.13 (NR) |
| SHOEBOX Audiometer25,26 | Online app that uses headphones (https://www.shoebox.md/products/shoebox-puretest) | > 40 db | 100 (81 to 100) | 96 (86 to 99) | 76 (59 to 88) | 100 (NR) |
| uHear 27 | Online app (https://apps.apple.com/us/app/uhear/id309811822) | > 40 dB | 100 (66 to 100) | 89 (77 to 96) | NR | NR |
| Whispered voice test (three studies, n = 296, pooled data) | Stand at arm's length behind the patient and have the patient block one ear; the clinician then whispers letter or number combinations Positive test: failure to repeat at least three of six combinations | > 40 dB | 46 (36 to 56) | 78 (68 to 86) | 2.08 (NR) | 0.69 (NR) |
dB = decibels; NR = not reported.
TABLE 3. Special Considerations Affecting Audiometry Interpretation
| Environment |
| Requires quiet testing room with sound-absorbing materials; sound levels should not exceed ANSI guidelines28 |
| Sound level can be measured to ensure specifications are met |
| Equipment |
| Must be calibrated annually according to ANSI specifications29 |
| Audiometer (hand-held, diagnostic), AudioScope30 |
| Transducers (circumaural or supra-aural headphones, insert earphones, bone oscillator) |
| Patient history |
| Accurate history can aid in identifying necessary accommodations during testing or help identify patients who may exaggerate hearing loss (intentionally or not), including patients with cognitive decline31,32 |
| Objective testing may be indicated if a reliable test cannot be measured and may also be appropriate for difficult-to-test populations33 |
| Recent noise exposure can affect test validity; avoid or minimize loud noise exposure at least 14 hours before testing34 |
| Personnel |
| Trained support personnel with direct supervision of an audiologist or physician—requirements may vary by state or local guidelines |
| Suggested guidelines are provided by the Academy of Audiology and American Speech-Language-Hearing Association35,36 |
| Physical findings |
| Anatomic anomalies (i.e., atresia, collapsed canals, stenosis), canal occlusion (i.e., cerumen impaction, foreign bodies, debris, infection), or eardrum perforation can affect testing results37 |
| Help determine site of lesion and appropriate transducer for testing; debridement may be indicated before testing to ensure accurate results38 |
ANSI = American National Standards Institute.
Before any testing, an otoscopic examination should be completed to evaluate the outer ear and external auditory canal and confirm visualization of a normal tympanic membrane. Pure-tone audiometry, using an audiometer, is the reference standard for hearing loss detection. It can be used for screening and comprehensive testing.39 An audiometer (handheld or tabletop) tests standard speech frequencies from 250 to 8,000 hertz. The handheld audiometer is typically used to screen limited frequencies, whereas a traditional table-top version is used for comprehensive audiologic testing. Both function by assessing various intensity levels (measured in decibels) and frequency (measured in hertz) for each ear independently. During testing, it is essential that the testing room is quiet for reliable results. Screening tests and pure-tone testing can be performed by a trained health care professional in the primary care setting or through referral to an audiologist or otolaryngologist.
Comprehensive and threshold search audiometry, performed by an audiologist, requires a soundproof room and longer testing time. By identifying the lowest hearing levels specific to frequency per ear, threshold audiometry defines the patient's severity of hearing loss and provides the data to program hearing aids. Comprehensive audiometry includes air and bone testing to distinguish between conductive, sensorineural, and mixed hearing loss paired with tympanometry, speech-reception thresholds, and word-recognition measures to complete a diagnostic hearing evaluation.40 The American Speech-Language-Hearing Association makes recommendations on how testing is performed and how thresholds are identified in a systematic way for reliability.13 Physicians should check with their state and local agencies for licensing requirements of audiometry personnel (https://www.asha.org/advocacy/state/).
Interpretation
Sound in everyday life is detected via air conduction through the outer, middle, and inner ears and related neural pathways. Bone conduction depends on the inner ear and neural pathways and is usually part of a comprehensive evaluation with an audiologist; it is not typically recorded during screening tests.41 Bone-conduction testing, which relies on methods similar to Weber and Rinne tuning fork tests (https://www.youtube.com/watch?v=K2uDW5CoGNY), must be performed to determine the type of hearing loss.41 Formal bone-conduction testing measures a pure-tone threshold by placing a device on the mastoid bone that sends sound directly to the inner ear.41
Pure-tone audiometry is recorded on a graph called an audiogram; Figure 1, Figure 2, and Figure 3 depict different audiograms.38 The horizontal axis shows recorded frequencies (hertz), shown from low pitches on the left to high pitches on the right. The vertical axis illustrates recorded intensity (decibels) from soft (top) to loud (bottom). Recorded thresholds lower on the graph generally indicate some degree of hearing loss; the softest sound a patient can hear 50% of the time is marked as a threshold.13 In the provided figures, a mark recorded with a blue X represents the left ear, and marks recorded with a red circle indicate the right ear. Most audiograms have a key for the symbols of the various tests the examiner will perform to display air-conduction testing vs. bone-conduction testing. A test called masking is performed if a large difference in responses between ears occurs to isolate the testing ear for more accurate measures.37 In the figures in this article, masked air-conduction testing is indicated by changing the blue X to a square and the red circle to a triangle; masked bone-conduction testing is presented with brackets.
FIGURE 1.
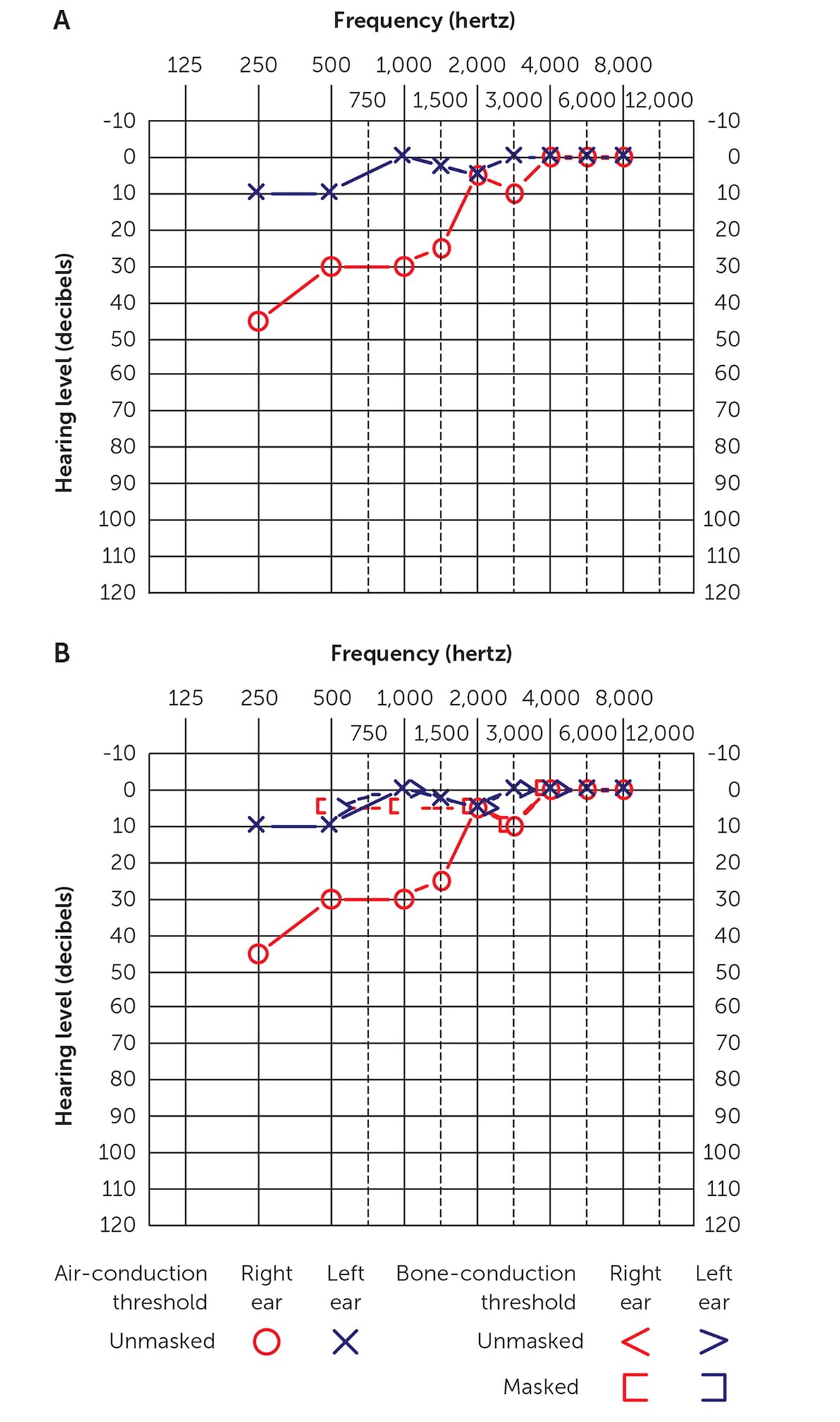
Audiograms. (A) Air conduction only; (B) air and bone conduction. Right ear: bone conduction is better than air conduction. The patient has low- to midfrequency conductive hearing loss because of tympanic membrane perforation.
Adapted with permission from Walker JJ, Cleveland LM, Davis JL, et al. Audiometry screening and interpretation. Am Fam Physician. 2013;87(1):44.
FIGURE 2.
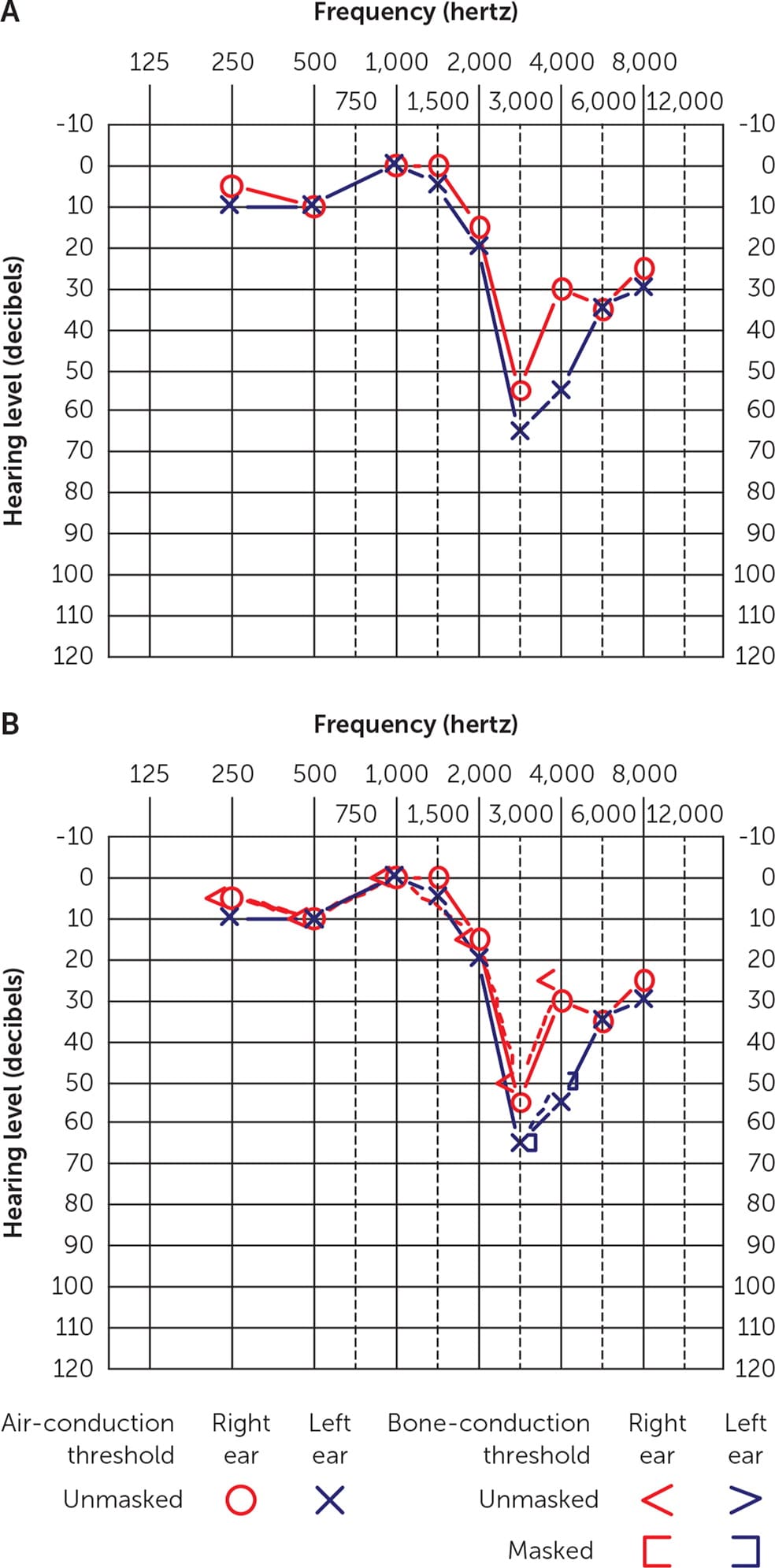
Audiograms. (A) Air conduction only; (B) air and bone conduction. Bilateral sensorineural hearing loss (noise induced). No significant differences are found between air- and bone-conduction thresholds. The asymmetry at 3,000 hertz and 4,000 hertz, with the left ear worse than the right ear, reflects this patient's occupation as an infantry soldier and a right-handed shooter. The relatively mild degree of asymmetry with the history of noise exposure does not, by itself, suggest a retrocochlear lesion.
Adapted with permission from Walker JJ, Cleveland LM, Davis JL, et al. Audiometry screening and interpretation. Am Fam Physician. 2013;87(1):45.
FIGURE 3.
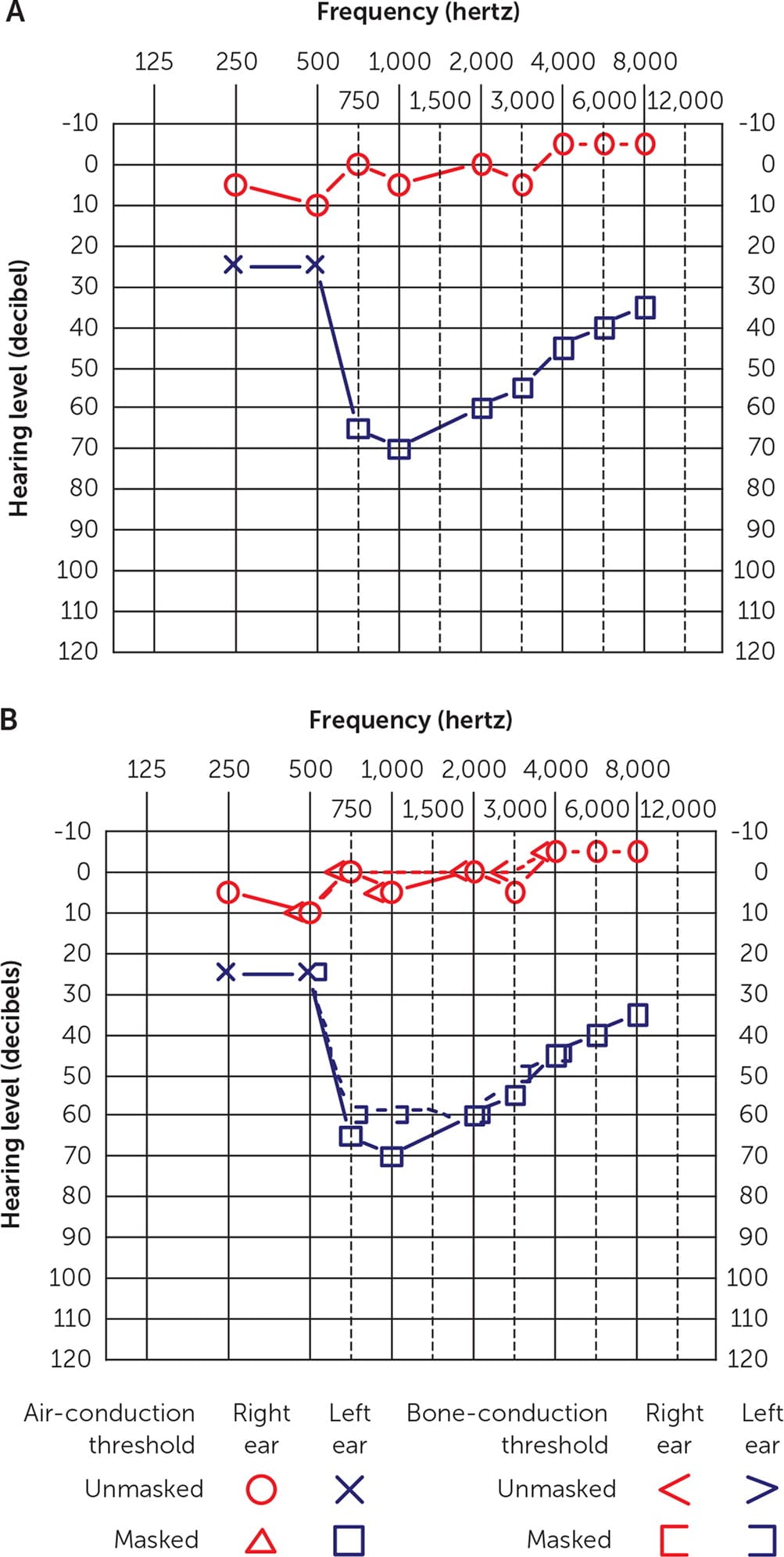
Audiograms. (A) Air conduction only; (B) air and bone conduction. Left ear unilateral sensorineural hearing loss due to vestibular schwannoma (retrocochlear). With sensorineural hearing loss, no significant difference occurs in the threshold between air- and bone-conduction.
Adapted with permission from Walker JJ, Cleveland LM, Davis JL, et al. Audiometry screening and interpretation. Am Fam Physician. 2013;87(1):45.
The three types of hearing loss are conductive, sensorineural, and mixed. Patients with outer- or middle-ear abnormalities may have a conductive loss (Figure 138 ), whereas patients with inner-ear damage (cochlear or nerve) may have a sensorineural hearing loss (Figure 238 ). A combination of conductive and sensorineural is called mixed hearing loss. Conductive or mixed hearing loss will show gaps between air- and bone-conduction thresholds, whereas sensorineural hearing loss does not.41 Audiograms that show a unilateral or asymmetrical sensorineural hearing loss can be signs of retrocochlear pathology (e.g., vestibular schwannoma) and warrant additional evaluation by an audiologist and otolaryngologist as well as imaging studies42 (Figure 338 ).
Coverage and Cost Considerations
A Medicare beneficiary can directly access an audiologist without needing a referral once every 12 months for nonacute hearing conditions, such as self-recognition of hearing loss. A patient using Medicare cannot self-refer to be prescribed, fit for, or to change hearing aids; an office visit to a physician, nurse practitioner, or physician's assistant is needed to document medical necessity (e.g., ensuring the appropriate diagnosis, review of the audiogram or audiology report) before an order for hearing aids can be placed.43 Historically, most commercial insurance payors did not cover the cost of hearing aids, although currently, some may include this benefit. Medicare Parts A and B do not pay for hearing aids,44 but some Medicare Advantage (Part C) or other supplemental plans may provide insurance coverage for hearing aids. For eligible hearing tests, Medicare Part B covers 80% of the Medicare-approved amount after an individual meets the Medicare deductible.45 Medicaid coverage for hearing aids varies by state, and patients should be advised to consult their individual policies to determine covered benefits.
In October 2022, the U.S. Food and Drug Administration approved over-the-counter hearing aids, which are substantially less expensive, for those 18 years and older with self-perceived mild to moderate hearing loss.46 An American Family Physician Curbside Consultation provides detailed information for family physicians about over-the-counter hearing aids.47 If severe hearing loss is suspected, patients should see their family physician or an otolaryngologist for an examination of their ears and obtain referral to an audiologist for a formal audiogram and hearing aid evaluation. If hearing loss is refractory to hearing aids, patients can be referred to an otolaryngologist to be evaluated for a cochlear implant, a surgically implanted device that directly stimulates the auditory nerve, if desired.12,48
Prevention
Hearing loss is progressive and usually not reversible; family physicians should counsel patients on the importance of protecting their hearing. The use of in-ear listening devices and occupational noise exposure increases the risk of developing hearing loss over time.49–51 Hearing protection (e.g., ear plugs, earmuffs) should be worn when experiencing loud noises in occupational and recreational settings to preserve hearing.52,53 The user should note a definite decrease in their perception of noise if these devices are fitted properly. Educational resources for physicians and patients on hearing conservation are found in eTable A.
eTABLE A Resources on Hearing Loss for Physicians and Patients
| Resource | Description |
|---|---|
| American Academy of Audiology https://www.audiology.org/consumers-and-patients/ | Overview of hearing, hearing loss, and hearing aids for patients, which includes help with finding an audiologist |
| American Academy of Otolaryngology–Head and Neck Surgery https://www.enthealth.org/be_ent_smart/otc-hearing-aids-faqs | Frequently asked questions for patients about OTC hearing aids |
| American Speech-Language-Hearing Association OTC hearing aid resources for primary care physicians https://www.asha.org/aud/otc-hearing-aid-toolkit/resources-for-physicians/ Patient hearing checklist https://www.asha.org/siteassets/audiology/patient-hearing-checklist.pdf | Summary helping physicians identify which patients would be good candidates for an OTC hearing aid Checklist for patients to identify concerns of hearing loss |
| Hearing Loss Association of America https://www.hearingloss.org | Organization that offers advocacy, support, and resources for people who have hearing loss |
| National Hearing Test https://www.nationalhearingtest.org/wordpress/?page_id=2730 | Validated home hearing test, available free for AARP members |
OTC = over the counter.
This article updates a previous article on this topic by Walker, et al.38
Data Sources: A PubMed search was completed in Clinical Queries using key terms hearing loss, hearing loss screening, masking and hearing loss, audiograms, and hearing loss prevention. The search included meta-analyses, randomized controlled trials, clinical trials, and review articles. Essential Evidence Plus was reviewed. Websites for the U.S. Preventive Services Task Force, the World Health Organization, the Centers for Disease Control and Prevention, the Agency for Healthcare Research and Quality evidence reports, the American Speech-Language-Hearing Association, AARP, CMS, American Academy of Audiology, the Hearing Loss Association of America, the American Academy of Otolaryngology–Head and Neck Surgery, Occupational Safety and Health Administration, and YouTube were also searched. Search dates: April, September, October 2023; February 2024.
