Obstructive sleep apnea (OSA) is a common disorder that affects quality of life and is associated with comorbidities such as hypertension, atrial fibrillation, heart failure, coronary heart disease, type 2 diabetes mellitus, and stroke. OSA is characterized by a reduction or cessation of breathing during sleep, resulting in intermittent hypoxemia, autonomic fluctuation, and sleep fragmentation. The U.S. Preventive Services Task Force states that there is insufficient evidence to recommend routine screening for OSA in the absence of symptoms. OSA should be considered in patients with excessive daytime fatigue, unrestful sleep, persistent snoring, and nocturnal awakenings with gasping or choking. The STOP-BANG questionnaire is the most sensitive screening tool for OSA, and the diagnostic standard is polysomnography with an observed apnea-hypopnea index greater than 5 in the presence of symptoms or greater than 15 without symptoms. Home sleep apnea testing is a useful diagnostic option in patients who have symptoms consistent with moderate to severe OSA without significant cardiopulmonary comorbidities. Positive airway pressure, with a humidified nasal or facial mask, is the first-line treatment for adults with OSA. Weight loss is a beneficial adjunct to treatment through intensive lifestyle modification, medications, or bariatric surgery. Alternatives for patients intolerant of or nonadherent to positive airway pressure include changing the type of mask used, mandibular advancement devices, hypoglossal nerve stimulation, and other surgical interventions. Although many OSA therapies effectively improve daytime sleepiness and blood pressure, none have demonstrated a mortality benefit in randomized controlled trials.
Obstructive sleep apnea (OSA) is a common disorder that causes functional impairment and decreased quality of life. As many as 17% of women and 34% of men in the United States have OSA, with rates increasing.1,2 OSA is characterized by a reduction or cessation of breathing during sleep that results in intermittent hypoxemia, autonomic fluctuation, and sleep fragmentation despite persistent respiratory effort, distinguishing OSA from central sleep apnea.1 OSA is clinically defined by the International Classification of Sleep Disorders, 3rd ed. (Table 1).3 Severity is determined by the apnea-hypopnea index (mild = 5 to 14 events per hour; moderate = 15 to 29 events per hour; severe = 30 or more events per hour).1,3,4 This article focuses on adults; a recent American Family Physician article details the evaluation and management of OSA in children.5
WHAT'S NEW ON THIS TOPIC
| Patients with severe obstructive sleep apnea have a two-fold greater risk of major adverse cardiovascular events and stroke, a nearly threefold greater risk of cardiac death, and a twofold increase in all-cause mortality. |
| A 2020 systematic review evaluated interventions to improve positive airway pressure usage in adults with obstructive sleep apnea. In positive airway pressure–naive patients, behavioral strategies yielded an increase in device use of 1.3 hours per night. |
SORT: KEY RECOMMENDATIONS FOR PRACTICE
OSA = obstructive sleep apnea; PAP = positive airway pressure.
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to https://www.aafp.org/afpsort.
TABLE 1. American Academy of Sleep Medicine International Classification of Sleep Disorders, 3rd Ed., Text Revision, for Obstructive Sleep Apnea
| A. The presence of at least one of the following: Symptoms of sleepiness, fatigue, insomnia, or other symptoms leading to impaired sleep-related quality of life Wakes short of breath, gasping, or choking Bed partner/observer reports habitual snoring or breathing interruptions during the patient's sleep |
| B. Polysomnography or home sleep apnea testing demonstrates: 5 or more predominantly obstructive respiratory events per hour of sleep/monitoring during polysomnography (obstructive and mixed apneas, hypopneas, or respiratory effort–related arousals) |
| C. Polysomnography or home sleep apnea testing demonstrates: 15 or more predominantly obstructive respiratory events per hour |
Note: Diagnostic of obstructive sleep apnea if criteria A and B are met or criterion C is met alone. The symptoms must not be better explained by another current sleep disorder, medical disorder, medication, or substance use.
Information from reference 3.
HEALTH DISPARITIES
Several studies have highlighted disparities in diagnosing OSA. When adjusting for confounding factors, underdiagnosis has been reported in Black and Hispanic patients, people who are uninsured, and women. Black patients are twice as likely as White patients to experience severe disease.2,6 OSA is underdiagnosed in pregnant women and is associated with maternal morbidity (e.g., preeclampsia, eclampsia, cardiomyopathy) and mortality.7 The American College of Obstetricians and Gynecologists recommends that pregnant patients with suspected OSA be referred to a sleep medicine specialist for evaluation and treatment.7
WHAT ARE THE MORBIDITY AND MORTALITY RISKS ASSOCIATED WITH OSA?
OSA is an independent risk factor for the development of hypertension, atrial fibrillation, heart failure, coronary heart disease, type 2 diabetes mellitus, and stroke. Increased OSA severity is associated with higher morbidity and mortality risks from comorbid conditions.1,8–10
Evidence Summary
OSA is associated with several comorbid conditions, particularly cardiovascular and metabolic disease, and independently increases the risk of coronary and cerebrovascular events such as myocardial infarction and stroke (Table 2).2,9–13 OSA that is increasing in severity is associated with worse control of comorbid conditions such as chronic obstructive pulmonary disease, heart failure, and atrial fibrillation.2,13 Patients with severe OSA have a two-fold greater risk of major adverse cardiovascular events and stroke, a nearly threefold greater risk of cardiac death, and a nearly twofold increase in all-cause mortality.2,8,14
TABLE 2. Prevalence of Obstructive Sleep Apnea With Comorbid Conditions
| Condition | Prevalence |
|---|---|
| Obesity-hypoventilation syndrome | 90% |
| Atrial fibrillation | 76% to 85% |
| Heart failure | 75% |
| Resistant hypertension | 73% to 82% |
| Referred to bariatric surgery | 71% to 77% |
| Stroke | 71% |
| Pulmonary hypertension | 70% to 80% |
| Type 2 diabetes mellitus | 65% to 85% |
| Idiopathic pulmonary fibrosis | 59% to 88% |
| Hypothyroidism | 50% |
| Posttraumatic stress disorder | 50% |
| Insomnia | 39% to 58% |
| Hypertension | 30% to 50% |
| Opioid therapy for chronic spinal pain | 14% |
| Major depressive disorder | 7% to 44% |
| Chronic obstructive pulmonary disease | 5% to 85%* |
*—Wide prevalence range attributed to differences in methodology and diagnostic and demographic criteria used.
WHAT SYMPTOMS ARE MOST PREDICTIVE OF OSA?
Excessive daytime fatigue and waking up feeling unrested are the most common presenting symptoms of OSA. Patients with these symptoms should be considered for a diagnostic evaluation.1,4,15
Evidence Summary
Table 3 provides common signs and symptoms of OSA and their associated sensitivity and specificity.1,2,4,12,15 Although snoring is highly sensitive for OSA, it is relatively nonspecific. Observed cessation of breathing during sleep is the most specific symptom, followed by nocturnal gasping or choking with awakenings.1,4,12,15 There are no specific physical examination findings that directly correlate to OSA; however, it is two times as common in people who are overweight and four times as common in people who are obese.1,12 Table 4 lists risk factors for the development of OSA.1,8,10–12
Several conditions may confound the diagnosis of OSA. Obesity-hypoventilation syndrome has the highest prevalence of coexisting OSA, with 90% of patients having OSA and 70% with severe OSA. Conversely, only 10% to 20% of patients with OSA have obesity-hypoventilation syndrome. Patients with obesity-hypoventilation syndrome have a higher risk of heart failure, pulmonary hypertension, hospitalization, and all-cause mortality than those with OSA.16 Several case reports have described OSA masquerading as narcolepsy or depression, and OSA should be considered when evaluating patients for these conditions.17,18
TABLE 3. Signs and Symptoms Associated With Obstructive Sleep Apnea
| Symptom | Prevalence | Apnea-hypopnea index sensitivity | Apnea-hypopnea index specificity |
|---|---|---|---|
| Excessive daytime sleepiness, fatigue, unrefreshing sleep | 73% to 90% | ≥ 5: 38% to 53% ≥ 15: 41% to 60% | ≥ 5: 59% to 78% ≥ 15: 52% to 71% |
| Snoring | 50% to 60% | ≥ 5: 79% to 97% ≥ 15: 77% to 96% | ≥ 5: 27% to 46% ≥ 15: 9.7% to 35% |
| Headaches on awakening > 50% of days | 12% to 18% | ≥ 5: 12% to 34% ≥ 15: 12% to 32% | ≥ 5: 91% to 95% ≥ 15: 82% to 88% |
| Nocturnal choking or gasping | 10% to 15% | ≥ 15: 34% to 70% | ≥ 15: 77% to 92% |
| Reported apnea | 10% to 15% | ≥ 15: 73% to 87% | ≥ 15: 33% to 51% |
| Nocturnal gastroesophageal reflux | 50% to 75% | — | — |
| Nocturia ≥ 2 times per night | 30% | — | — |
| Impaired cognition | 26% | — | — |
| Mood changes | 20% to 40% | — | — |
TABLE 4. Risk Factors for the Development of Obstructive Sleep Apnea and Associated Comorbid Diagnoses
| Risk factor | Odds ratio |
|---|---|
| Age 40 to 70 years | 1.4 to 3.2 |
| Atrial fibrillation* | 4.0 |
| Craniofacial abnormalities* | Unknown |
| Diabetes mellitus* | 1.2 to 2.6 |
| Enlarged upper airway soft tissues* | Unknown |
| Heart failure* | 2.4 |
| History of stroke* | 1.6 to 4.3 |
| Hypertension* | 1.4 to 4.9 |
| Male sex | 1.7 to 3.0 |
| Obesity | 4.0 to 10.5 |
| Postmenopausal | 2.8 to 4.3 |
Note: Odds ratio represents the odds of having a condition plus obstructive sleep apnea vs. having the condition alone.
*—Conditions associated with obstructive sleep apnea. Meta-analyses have not identified a causal link.
WHAT ARE THE RECOMMENDED SCREENING AND DIAGNOSTIC TESTS FOR OSA?
The STOP-BANG questionnaire is the most sensitive and widely used screening tool for OSA1,19,20 (Figure 120). Although sleep laboratory–based polysomnography is considered the diagnostic standard, home sleep apnea testing is recommended by the American Academy of Sleep Medicine for patients with symptoms consistent with moderate to severe OSA without significant cardiopulmonary disease.1,4,21,22
FIGURE 1. STOP-Bang Questionnaire
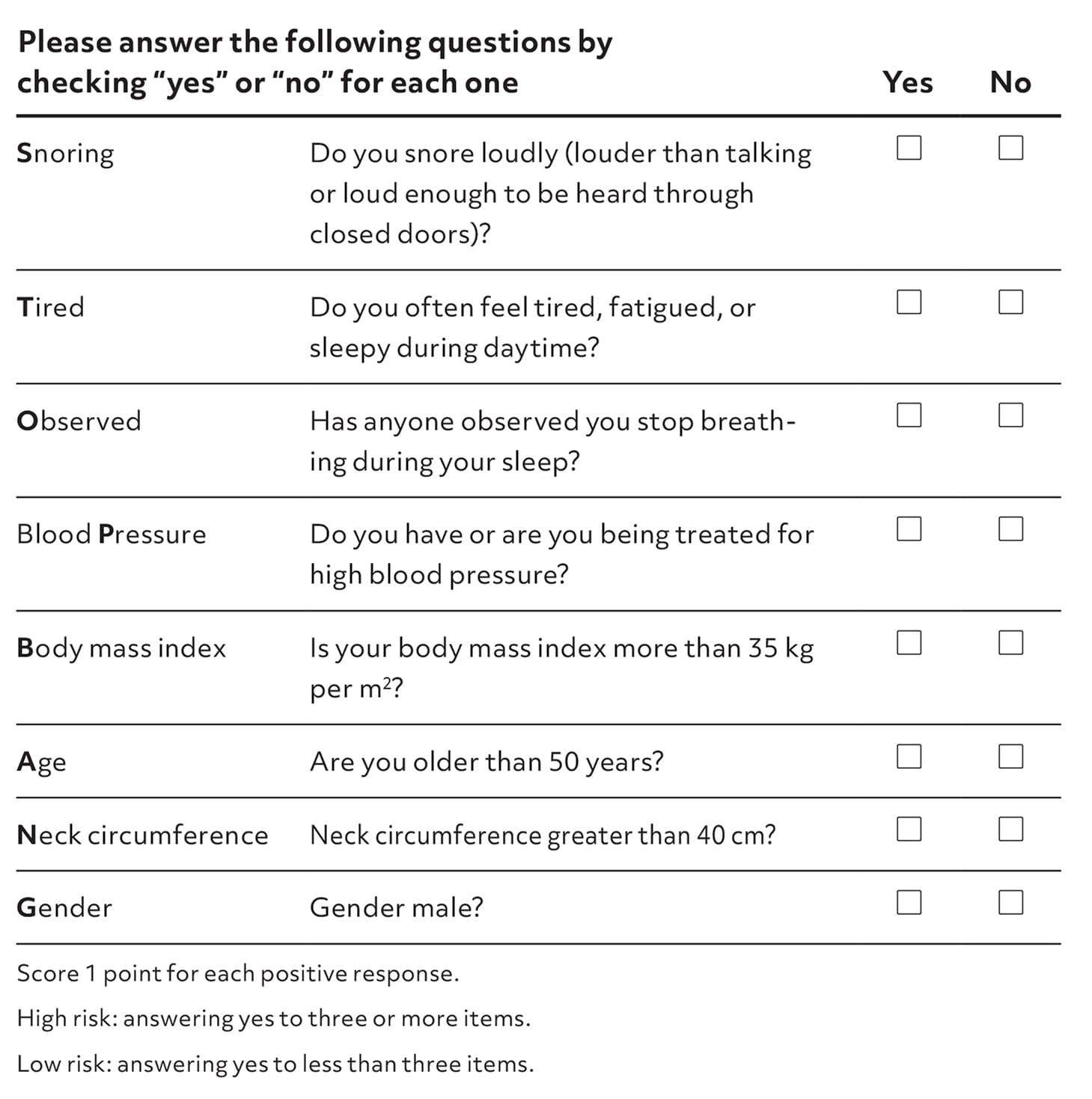
STOP-BANG questionnaire to assess the risk of obstructive sleep apnea.
Adapted with permission from Chung F, Yegneswaran B, Liao P, et al. STOP questionnaire: a tool to screen patients for obstructive sleep apnea. Anesthesiology. 2008;108(5):821.
Evidence Summary
Options for OSA screening include the STOP-BANG and Berlin questionnaires, with sensitivities of 90% and 77%, respectively.1,19,20 Although the Epworth Sleepiness Scale can help characterize the degree of daytime sleepiness, its low sensitivity (47%) limits its use.19
The American Heart Association suggests assessing for OSA in people with poorly controlled hypertension, heart failure, pulmonary hypertension, nocturnal angina, and recurrent atrial fibrillation.1,2 An expert consensus statement recommends that pregnant patients who have a body mass index (BMI) greater than 30 kg per m2 or a history of hypertension or diabetes be screened for OSA, ideally in the first trimester.23 For all patients, in the absence of symptoms, the U.S. Preventive Services Task Force states that there is insufficient evidence to recommend routine screening for OSA.8
Polysomnography is most often conducted in a sleep laboratory, which can be costly (up to $1,300) and involve significant wait times for patients.22 Home-based testing costs less ($230), is more convenient for patients, and may reduce patient anxiety compared with polysomnography, and has an 80% sensitivity.12,16,21,22 Figure 2 outlines a diagnostic approach to OSA.4
FIGURE 2.
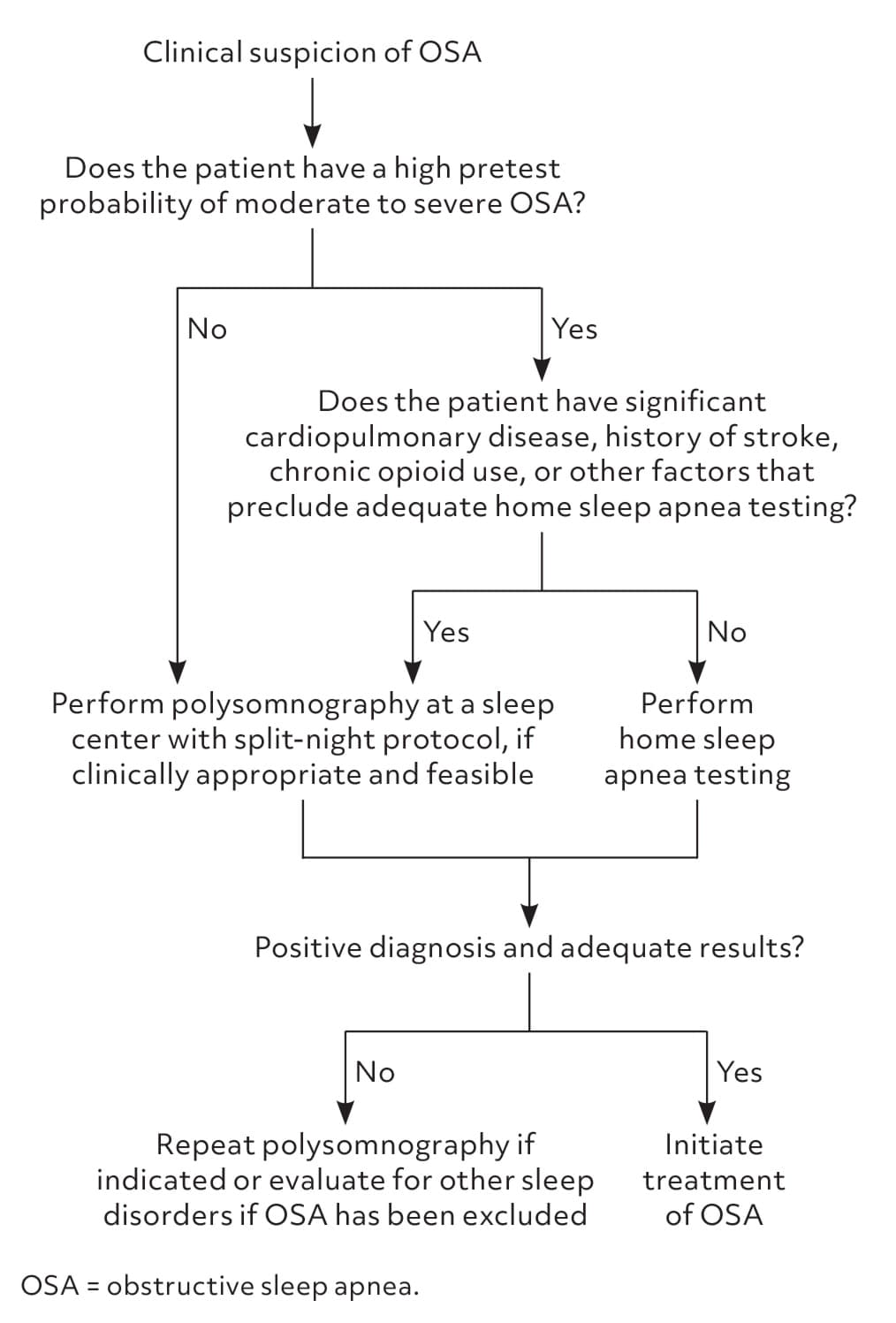
Simplified algorithm for diagnostic testing of obstructive sleep apnea.
Adapted with permission from Kapur VK, Auckley DH, Chowdhuri S, et al. Clinical practice guideline for diagnostic testing for adult obstructive sleep apnea: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2017;13(3):487.
WHAT ARE THE BENEFITS OF POSITIVE AIRWAY PRESSURE TREATMENT IN PATIENTS WITH OSA AND WHEN SHOULD IT BE INITIATED?
Positive airway pressure (PAP) therapy improves OSA severity, blood pressure, daytime sleepiness, and sleep-related quality of life; however, it does not reduce cardiovascular events or all-cause mortality.24,25 All patients with symptomatic OSA and all asymptomatic patients with an apnea-hypopnea index greater than 15 events per hour should be offered treatment with PAP.1,24
Evidence Summary
A meta-analysis found that PAP treatment of OSA improves disease severity (i.e., a reduction of an apnea-hypopnea index by 23 events per hour), daytime sleepiness (i.e., a reduction in Epworth Sleepiness Scale by 2.4 points), and blood pressure (i.e., a reduction of 24-hour values by 1.5 mm Hg).24 Randomized controlled trials found no change in cardiovascular events with PAP therapy.25 Although observational data have suggested that PAP therapy may be associated with a reduction in all-cause mortality, randomized controlled trials have not confirmed this benefit. Concerns of abbreviated PAP usage in the study population (i.e., an average of 3.3 hours per night) in one of the largest trials could explain the nonsignificant findings.24–26
The American Academy of Sleep Medicine and U.S. Department of Veterans Affairs/U.S. Department of Defense recommend that all patients with symptoms of OSA, and those without symptoms but with an apnea-hypopnea index greater than 15 events per hour, should be offered initial treatment with PAP. This recommendation is based on data showing increased morbidity risks and improved outcomes with treatment in these patient populations. 1,24
WHAT ARE EVIDENCE-BASED TECHNIQUES FOR IMPROVING PAP ADHERENCE IN PATIENTS?
Education, support, and behavioral interventions can improve PAP usage, especially those requiring active patient participation.1,27 Heated air humidification and the use of nasal masks are associated with higher PAP adherence.28 Bilevel and auto-titrating PAP have limited outcome benefits compared with fixed-pressure continuous PAP.1,24
Evidence Summary
Patients who use PAP longer on average each night have better outcomes.1,24 A recent large systematic review evaluated interventions to improve PAP usage in adults with OSA and found that behavioral strategies yielded an increase in device usage of 1.3 hours per night in PAP-naive patients.27
Randomized controlled trial data investigating the differences between PAP interfaces are limited; however, patients prefer nasal masks, and humidified air may reduce nasal symptoms. Both interventions increase PAP usage by 30 minutes per night, but neither has demonstrated improvements in daytime sleepiness, or quality of life, or a reduced apnea-hypopnea index.1,24,28 Bilevel and auto-titrating PAP do not improve OSA severity, treatment adherence, daytime sleepiness, or quality of life compared with fixed-pressure CPAP but may have separate indications.1,24 In patients intolerant of PAP, alternative treatments should be offered.1,24 Table 5 outlines treatment options for OSA.24,29–43 For all patients, treatment choice should be based on clinical evaluation, comorbidities, and preference.
TABLE 5. Treatment Options for Obstructive Sleep Apnea
| Therapy | Indications | Risks | Summary of evidence |
|---|---|---|---|
| Fixed-pressure CPAP | All patients with symptomatic OSA or asymptomatic OSA with an apnea-hypopnea index greater than 15 events per hour | Modest weight gain (increase in BMI of 0.15 kg per m2), oral or nasal dryness, nonadherence rates up to 50% | Apnea-hypopnea index reduction of 23 events per hour Epworth Sleepiness Scale score reduction of 2.4 points Modest improvement in sleep-related quality of life (Functional Outcomes of Sleep Questionnaire [5- to 20-point scale]/Sleep Apnea Quality of Life Index) No effect on overall quality of life (36-item short-form survey [0 to 100 score for each component]) Reduction in 24-hour systolic and diastolic blood pressure (−1.5 mm Hg/−1.6 mm Hg) No effect on neurocognitive function, mood, A1C, hospitalizations, or left ventricular ejection fraction No randomized controlled trial data of effect on cardiovascular event rate or all-cause mortality |
| Adjunctive upper airway surgery for PAP tolerance | Moderate to severe OSA, intolerant of PAP, or with pressure-related adverse effects when using PAP | Epistaxis, hematoma, infection, loss of smell, nasal congestion, saddle nose deformity, septal perforation | Mostly lower-quality, observational evidence Apnea-hypopnea index reduction of 22.9 events per hour Epworth Sleepiness Scale score reduction of 6 points Improved CPAP adherence by 2.2 hours per night May increase PAP use from 39% to 90% |
| Auto-titrating PAP | Not generally recommended over fixed-pressure CPAP | Similar to fixed-pressure CPAP; increased cost | No difference in disease- or patient-oriented outcomes compared with fixed-pressure CPAP |
| Bariatric surgery | Adults with BMI ≥ 35 kg per m2 or BMI ≥ 30 kg per m2 with comorbidities (including OSA) | < 0.5% mortality risk, infection, anastomotic leak and ulceration, nutritional deficiency | Apnea-hypopnea index reduction of 25 events per hour compared with conservative weight-loss management Epworth Sleepiness Scale score reduction of 5.6 points Reduction in systolic and diastolic blood pressure (9.3 mm Hg/6.9 mm Hg) > 97% of patients still had residual OSA (apnea-hypopnea index > 5 events per hour) after bariatric surgery |
| Bilevel PAP | Not generally recommended over CPAP; consider in cases of nonadherence | Adverse effects similar to CPAP; increased cost | Bilevel PAP may reduce apnea-hypopnea index by 2.2 events per hour over CPAP Improved adherence by 0.8 hours per night in those nonadherent to CPAP therapy (no difference when used as first-line treatment) No difference in patient-oriented outcomes between CPAP and bilevel PAP |
| Hypoglossal nerve stimulation | Moderate to severe OSA, nonadherent to PAP, BMI ≤ 32 kg per m2 | Low risk of serious adverse events (< 2%); tongue or lip weakness, pneumothorax, infection, scarring | No comparison to CPAP (studies in patients intolerant of or nonadherent to PAP therapy) Apnea-hypopnea index reduction of 24.9 events per hour Epworth Sleepiness Scale score reduction of 5 points |
| Lifestyle interventions | Recommended for all patients as an adjunct to OSA treatment | None | Apnea-hypopnea index reduction of 6 events per hour Epworth Sleepiness Scale score reduction of 1 point (for interventions resulting in an average reduction in BMI of 2.3 kg per m2) |
| Mandibular advancement devices (i.e., oral appliances) | Mild to moderate OSA, nonadherent to or intolerant of CPAP | Dental discomfort, temporomandibular joint pain, dry mouth, gum irritation, bruxism; low risk of discontinuation (50% lower discontinuation rate than CPAP) | Apnea-hypopnea index reduction of 13.6 events per hour (CPAP has 6.2 events per hour more than mandibular advancement devices) Epworth Sleepiness Scale score reduction of 3.8 points (similar to CPAP) Mandibular advancement device adherence better than CPAP by 0.7 hour per night Customized, titratable mandibular advancement devices better than off-the-shelf devices |
| Maxillomandibular advancement surgery | Moderate to severe OSA, nonadherent to PAP | Facial paresthesias, malocclusion, trismus, unfavorable cosmesis, hardware extrusion, infection, malunion | Mostly lower-quality, observational evidence Apnea-hypopnea index reduction of 44.9 to 47.8 events per hour Epworth Sleepiness Scale score reduction of 5.6 to 10.3 points May improve sleep-related quality of life by 3.5 points (Functional Outcomes of Sleep Questionnaire [5- to 20-point scale]) Reduction in systolic and diastolic blood pressure (6.3 mm Hg/2.7 mm Hg) |
| Myofunctional therapy (oral or tongue exercises) | Only recommended as salvage or adjunctive therapy | None reported | Low-quality evidence Apnea-hypopnea index reduction of 6 to 13.2 events per hour Epworth Sleepiness Scale score reduction of 3 to 4.5 points |
| Pharmacologic agents (i.e., solriamfetol [Sunosi], modafinil) | Refractory daytime sleepiness despite appropriate OSA treatment | Headache, insomnia, anxiety Discontinuation risk: 1.5% to 6.3% No evidence of serious adverse events | Inadequate evidence to support medications as primary OSA treatment Solriamfetol: Epworth Sleepiness Scale score reduction of 3.9 points Modafinil: Epworth Sleepiness Scale score reduction of 2.3 points |
| Positional therapy (i.e., lumbar/abdominal binders, semirigid backpacks, full-length pillows, tennis ball attached to patient's back, or alarms indicating change in position) | Only recommended as salvage or adjunctive therapy | None reported | Low-quality evidence Apnea-hypopnea index reduction of 7.4 events per hour |
| Uvulopalatopharyngoplasty surgery | Moderate to severe OSA, nonadherent to PAP | Throat pain, dysphagia, dysphonia, dysgeusia, tongue paresthesia, bleeding, airway compromise, or respiratory crisis | Mostly lower-quality, observational evidence Less effective than maxillomandibular advancement surgery Apnea-hypopnea index reduction of 12 to 15 events per hour May improve sleep-related quality of life by 3.5 points Reduction in systolic and diastolic blood pressure (6.3 mm Hg/2.7 mm Hg) Effectiveness may wane over time |
BMI = body mass index; CPAP = continuous positive airway pressure; OSA = obstructive sleep apnea; PAP = positive airway pressure.
WHAT ADDITIONAL THERAPIES ARE EFFECTIVE IN TREATING OSA?
Customized, titratable mandibular advancement devices are an alternative treatment option for patients with mild to moderate OSA who are nonadherent to PAP therapy.1,29 Lifestyle interventions have a modest impact on OSA outcomes and should be recommended for all patients.1,30,31 Wakefulness-promoting agents may be used to treat refractory sleepiness in patients with OSA adequately managed with PAP.31,32
Evidence Summary
Mandibular advancement devices (i.e., oral appliances) effectively treat OSA and reduce daytime sleepiness. Although less effective than PAP, they are associated with improved patient satisfaction and adherence rates.1,29,33 Weight loss through lifestyle interventions can result in modest improvements in the apnea-hypopnea index and Epworth Sleepiness Scale score.1,30,31 Positional and myofunctional therapy modestly improve OSA severity and daytime sleepiness, but the evidence is limited and of low quality.11,34,35 The available evidence on medications for the primary treatment of OSA is limited, low quality, and does not support their use.36 Wakefulness-promoting agents, such as solriamfetol (Sunosi) and modafinil, are effective in reducing daytime sleepiness in patients with refractory symptoms despite adequate PAP therapy, with their use limited by availability, adverse effects, and clinician experience.32
WHEN SHOULD PHYSICIANS REFER PATIENTS FOR SURGICAL TREATMENT OF OSA?
Most patients with OSA should have an initial trial of PAP therapy before considering surgical options. Referral may be considered in patients intolerant of PAP or as an adjunct when PAP is inadequate.1,24,37 Hypoglossal nerve stimulation surgery is reasonable in patients with moderate to severe OSA and a BMI of 32 kg per m2 or less.1,37 Physicians should consider referring patients for upper airway surgery if pressure-related adverse effects interfere with PAP use. In patients with obesity and OSA who qualify, bariatric surgery can improve OSA-related outcomes.37,44
Evidence Summary
The American Academy of Sleep Medicine recommends an initial trial of PAP therapy for all adults with OSA before consideration of surgical options, even in patients with noticeable anatomic abnormalities.37 Surgical intervention for sleep apnea should be considered in three clinical scenarios: salvage therapy for those who are intolerant of PAP, adjunct therapy to improve PAP effectiveness or adherence, and weight loss surgery.37
The most prominently studied surgical procedures are hypoglossal nerve stimulation, maxillomandibular advancement, and uvulopalatopharyngoplasty. Observational data have demonstrated that these procedures can reduce the apnea-hypopnea index, improve the Epworth Sleepiness Scale score, and modestly improve sleep-related quality of life.37–41 Overall, hypoglossal nerve stimulation is the safest and best-studied intervention, but studies have included only patients with moderate to severe OSA who were nonadherent to PAP therapy and had a BMI of 32 kg per m2 or less.38 Maxillomandibular advancement appears to be more effective than uvulopalatopharyngoplasty and has longer-lasting benefits.37,41
In patients with congestion or pressure-related adverse effects of PAP therapy, nasal, tonsillar, or palatal surgeries may increase PAP adherence by 50%, improve usage by 2 additional hours per night, and moderately improve sleep-related quality of life, apnea-hypopnea index, and Epworth Sleepiness Scale scores.37,42
Bariatric surgery has been associated with a reduction in OSA severity, daytime sleepiness, and blood pressure; however, it should be considered as an adjunct because OSA remission from weight loss surgery alone is rare.37,43,44
Data Sources: A PubMed search was completed in Clinical Queries using the key terms obstructive sleep apnea with incidence, prevalence, prevention, comorbidities, diagnostic mimics, morbidity, mortality, practice guidelines, therapy, diagnosis, and treatment. The search included meta-analyses, randomized controlled trials, clinical trials, clinical practice guidelines, and reviews. The Agency for Healthcare Research and Quality Effective Healthcare Reports, the Cochrane database, DynaMed, and Essential Evidence Plus were also searched. Search dates: May 4 to July 4, 2023, and May 2, 2024.
The opinions and assertions contained herein are the private views of the authors and are not to be construed as official or as reflecting the views of the U.S. Air Force, the Uniformed Services University of the Health Sciences, the U.S. Department of Defense, or the U.S. government.
