In the United States, 10% to 15% of adults are affected by gallstones, and cholesterol gallstones are the most prevalent subtype. Risk factors for developing gallstone disease include female sex; older age; certain medications; and having type 2 diabetes mellitus, nonalcoholic fatty liver disease, obesity, rapid weight loss, or hemolytic anemia. Nearly 80% of gallstones are found incidentally and remain asymptomatic. When symptomatic, gallstone disease usually presents as sudden onset right upper quadrant or epigastric abdominal pain. Common complications of gallstones include cholecystitis, choledocholithiasis, gallstone pancreatitis, and ascending cholangitis. The Murphy sign is a specific physical examination finding for acute cholecystitis. Ultrasonography is the initial imaging choice for detecting gallstones and acute cholecystitis. A hepatobiliary iminodiacetic acid (HIDA) scan can be used to evaluate for cholecystitis in patients with negative or equivocal ultrasound findings. Magnetic resonance cholangiopancreatography (MRCP) is an accurate, noninvasive diagnostic test to identify choledocholithiasis, certain malignancies, and biliary obstruction. Nonsteroidal anti-inflammatory drugs are safe and effective in treating pain from acute cholecystitis and biliary colic. Laparoscopic cholecystectomy is the treatment of choice for most patients with biliary colic or acute cholecystitis. Ursodeoxycholic acid and chenodeoxycholic acid should not routinely be used to treat gallstone disease, but they can be used as a nonsurgical alternative for certain patients. Postcholecystectomy syndrome is a potential postoperative complication that presents with abdominal pain, bloating, and diarrhea. (Am Fam Physician. 2024;109(6):518-524. Copyright © 2024 American Academy of Family Physicians.)
Gallstones, or cholelithiasis, are highly prevalent, affecting an estimated 10% to 15% of U.S. adults.1,2 Approximately 80% of all gallstones are cholesterol gallstones, which form because of precipitation of cholesterol.1,3 Black pigment gallstones (10% to 15%) comprise calcium bilirubinate, formed from unconjugated bilirubin deposition, often secondary to chronic hemolysis.2,3 Brown pigment stones (5%) are usually associated with biliary infections.3 Evidence-based answers to common questions about gallstone disease are discussed in this article.
WHAT'S NEW ON THIS TOPIC
| Recent meta-analyses have shown that dipeptidyl-peptidase-4 inhibitors (odds ratio = 1.22) and glucagon-like peptide-1 receptor agonists (relative risk = 1.27) increase the risk of gallstone disease, with greater risk in patients with longer duration of use (longer than 26 weeks). |
| A 2016 Cochrane review showed that nonsteroidal anti-inflammatory drugs provide greater relief from biliary pain compared with placebo (number needed to treat = 3) and antispasmodics (number needed to treat = 3) and no difference in pain control compared with opiates. |
| A systematic review of patients who underwent cholecystectomy found that 13% developed postcholecystectomy diarrhea. |
SORT: KEY RECOMMENDATIONS FOR PRACTICE
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease- oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to https://www.aafp.org/afpsort.
Who Is at Risk of Developing Gallstones?
Risk factors for developing gallstones include female sex; older age; certain medications; and having type 2 diabetes mellitus, nonalcoholic fatty liver disease, obesity, rapid weight loss, pregnancy, previous bariatric surgery, and hemolytic anemia (Table 14–9 ).
TABLE 1. Risk Factors for Developing Gallstones
| Chronic disease Dyslipidemia Hemolytic anemia Nonalcoholic fatty liver disease Obesity Type 2 diabetes mellitus Demographics Female sex Older age | Lifestyle Diet high in calories and refined carbohydrates Low physical activity levels Pregnancy Rapid weight loss (including after bariatric surgery) Medications Dipeptidyl-peptidase-4 inhibitors Estrogen-based therapy Glucagon-like peptide-1 receptor agonists |
EVIDENCE SUMMARY
Several large meta-analyses have shown that metabolic diseases, such as type 2 diabetes (relative risk = 1.65) and nonalcoholic fatty liver disease (odds ratio = 1.55), increase the risk of gallstones.6,10 Body mass index is associated with a nonlinear increased risk for gallstones, with greatest risk in those with a body mass index greater than 35 kg per m2 (odds ratio = 4.57).11 Dipeptidyl-peptidase-4 inhibitors and glucagon-like peptide-1 receptor agonists are often used in patients with metabolic disease, and recent meta-analyses have shown that dipeptidyl-peptidase-4 inhibitors (odds ratio = 1.22) and glucagon-like peptide-1 receptor agonists (relative risk = 1.27) increase the risk of gallstone disease, with greater risk in those with longer duration of use (longer than 26 weeks).7,8
Similarly, patients with rapid weight loss after having bariatric surgery have a greater risk of developing gallstones, with approximately 22% developing stones and the highest prevalence found in those who had a sleeve gastrectomy.9 Additionally, it is estimated that 12% of pregnant women have gallstones, and approximately 3% of those women require intrapartum cholecystectomy.12 Data from the Women's Health Initiative showed that women who take estrogen-based therapy have a greater risk for gallstones, leading to cholecystectomy (number needed to harm = 322).13 Patients with hemolytic anemia are also at risk for gallstone disease from hemoglobin degradation, which increases the risk of black pigment gallstones.14
What Are Common Complications in Patients With Gallstone Disease?
Complications include acute cholecystitis, choledocholithiasis, gallstone pancreatitis, and ascending cholangitis.
EVIDENCE SUMMARY
Approximately 20% of patients with gallstone disease develop complications.15 The complications are caused by the distal movement of gallstones into the cystic or common bile duct.1 The most common complication is acute cholecystitis; it occurs when a gallstone obstructs the cystic duct, resulting in bile retention and subsequent gallbladder inflammation.
Choledocholithiasis is the presence of gallstones in the common bile duct and occurs in 10% to 20% of patients with symptomatic gallstones.16 Common bile duct stones can result in complications (e.g., gallstone pancreatitis, ascending cholangitis).1 Gallstone pancreatitis occurs when a stone obstructs the sphincter of Oddi, resulting in epigastric pain and subsequently elevated pancreatic enzymes.1 Ascending cholangitis occurs because of the obstruction of bile flow, leading to a bacterial invasion from the small bowel into the biliary tract. Cholangitis can cause critical illness and commonly presents with fever, jaundice, and right upper quadrant pain.16 Figure 1 illustrates guidance for management of gallstone disease.1
FIGURE 1.
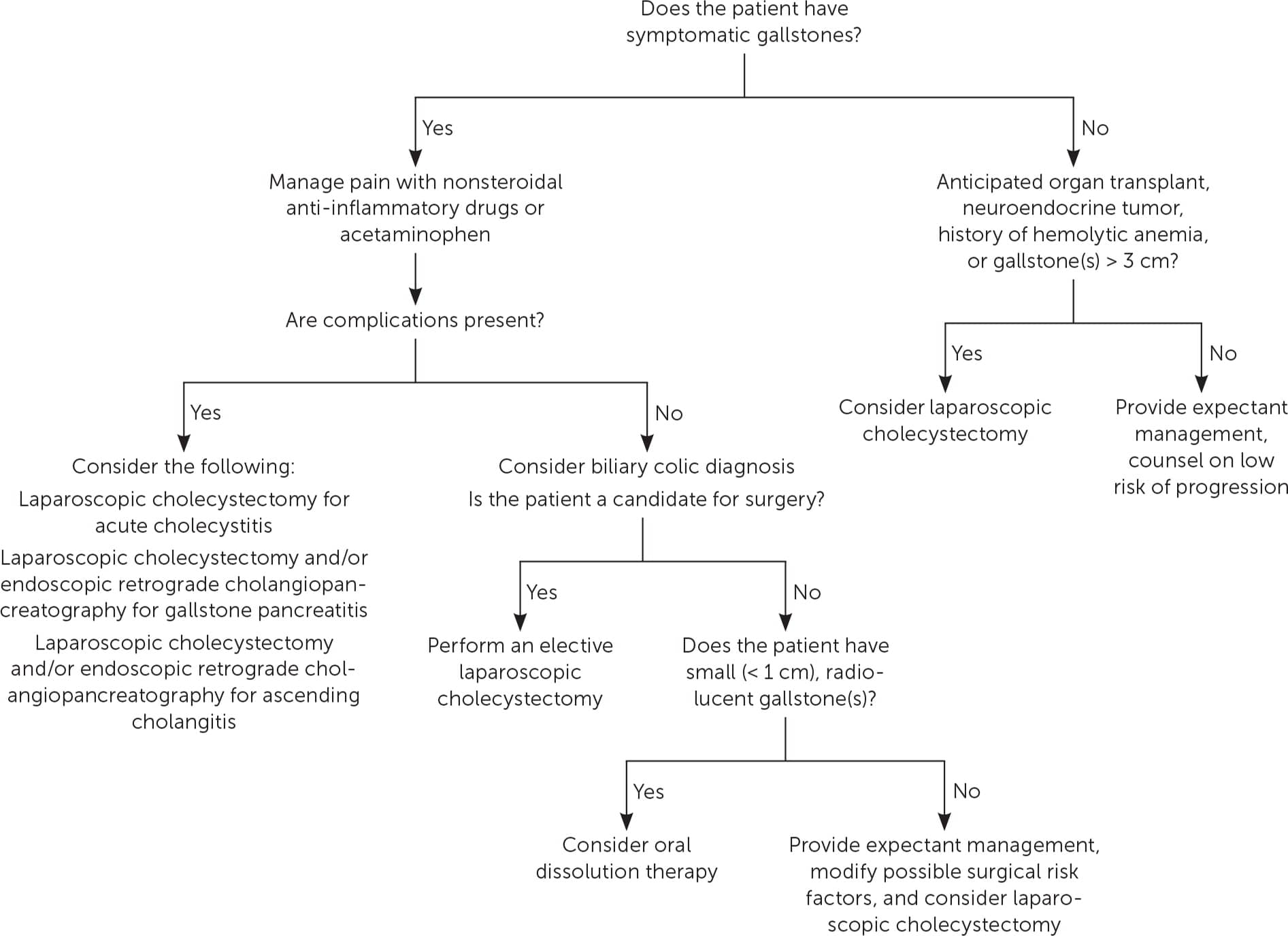
Management of gallstone disease.
Adapted with permission from Abraham S, Rivero HG, Erlikh IV, et al. Surgical and nonsurgical management of gallstones. Am Fam Physician. 2014;89(10):798.
Which Clinical Findings Suggest Gallstones and Their Complications?
Gallstone complications (e.g., biliary colic, cholecystitis, choledocholithiasis) can present with acute onset, continuous right upper quadrant or epigastric abdominal pain. The Murphy sign (inspiratory arrest during examiner-performed right upper quadrant palpation) is a specific examination finding for acute cholecystitis.
EVIDENCE SUMMARY
Symptomatic gallstone disease is usually associated with biliary tract obstruction. Transient gallstone obstruction can lead to biliary colic, whereas persistent obstruction causes acute cholecystitis. Pain from biliary colic peaks 1 hour after obstruction and usually resolves within 5 hours, whereas pain from cholecystitis persists beyond 6 hours.1,2
Cholecystitis and biliary colic present with sudden onset of right upper quadrant or epigastric pain that is intense, steady, and often occurs after fatty food intake.1 Although fever, emesis, rebound tenderness, jaundice, and leukocytosis may occur with cholecystitis, the likelihood ratios (LRs) for these findings are nonsignificant.17,18 The Murphy sign is a specific finding during physical examination for cholecystitis (LR+ = 11.5 to 21.3).17 Overall clinical gestalt has been shown to be most helpful in detecting cholecystitis, with a LR+ between 25 and 30.18 Patients with choledocholithiasis are more likely to have elevated bilirubin, gamma-glutamyl transpeptidase, or alkaline phosphatase levels (odds ratio = 3.0).19,20
Which Imaging Tests Should Be Used to Diagnose Gallstones and Acute Cholecystitis?
Right upper quadrant ultrasonography is recommended to initially detect gallstones and acute cholecystitis. A hepatobiliary iminodiacetic acid (HIDA) scan may be helpful in symptomatic patients with negative or equivocal right upper quadrant ultrasound findings.
EVIDENCE SUMMARY
The American College of Radiology Appropriateness Criteria recommend right upper quadrant ultrasonography as the first-line test in patients with right upper quadrant abdominal pain.21 Ultrasonography remains the test of choice because it is relatively affordable, accurate, rapidly performed, and radiation-free.21 One systematic review demonstrated that clinician-performed bedside point-of-care ultrasonography should also be considered to identify gallstones (LR+ = 7.5; LR− = 0.1).22
In patients with a high likelihood of cholecystitis and negative or equivocal ultrasound results, HIDA scanning should be the next step to evaluate for acute cholecystitis. A 2012 meta-analysis found that HIDA scans are more accurate (LR+ = 10.1; LR− = 0.1) than right upper quadrant ultrasonography (LR+ = 4.8; LR− = 0.2) and computed tomography (LR+ = 2.3; LR− = 0.1).23 However, HIDA scanning requires several hours to complete, is expensive, and does not identify extrabiliary causes of pain.21 Computed tomography is commonly performed for undifferentiated abdominal pain in the emergency department and is sensitive for detecting gallstones; however, it is costly, involves radiation exposure, and may miss noncalcified gallstones.21
Which Imaging Tests Should Be Used to Diagnose and Evaluate Choledocholithiasis?
Ultrasonography, magnetic resonance cholangiopancreatography (MRCP), and endoscopic ultrasonography can identify choledocholithiasis. Ultrasonography is commonly used given its wider availability and lower cost; MRCP and endoscopic ultrasonography are more accurate than ultrasonography in identifying choledocholithiasis. MRCP is less invasive than endoscopic ultrasonography but is expensive and may not be readily available. Although endoscopic ultrasonography is invasive, it can be diagnostic and therapeutic when patients are simultaneously undergoing endoscopic retrograde cholangiopancreatography.
EVIDENCE SUMMARY
As an initial imaging modality, ultrasonography can identify choledocholithiasis and common bile duct dilation but is limited in detecting other potential causes of biliary obstruction.24 A Cochrane review found that ultrasonography had a LR+ of 8.1 and LR− of 0.3 when evaluating for choledocholithiasis.25 Although much more expensive than ultrasonography, MRCP has a higher sensitivity (84%) and specificity (92%) in detecting choledocholithiasis.24,26 Furthermore, MRCP can detect other causes of biliary obstruction and pancreatic or biliary malignancies.24
In contrast, endoscopic ultrasonography provides slightly greater sensitivity (94%) and similar specificity (89%) in detecting choledocholithiasis and has the advantage of simultaneously being able to perform therapeutic endoscopic retrograde cholangiopancreatography to remove biliary stones, place a stent, or biopsy a mass.1,26 However, endoscopic ultrasonography and endoscopic retrograde cholangiopancreatography are invasive procedures, with 4% to 10% of patients developing complications such as pancreatitis, acute cholangitis, bowel perforation, or hemorrhage.1
Which Pain Management Options Are Safe and Effective in Patients With Biliary Colic or Cholecystitis?
Nonsteroidal anti-inflammatory drugs are a safe and effective treatment for acute biliary pain. Nonsteroidal anti-inflammatory drugs and intravenous lidocaine are non-inferior to opiates, and the use of opiates should be limited because of potential adverse effects.
EVIDENCE SUMMARY
A 2016 Cochrane review showed that nonsteroidal anti-inflammatory drugs provide greater relief of biliary pain compared with placebo (number needed to treat [NNT] = 3) and antispasmodics (NNT = 3), with no difference in pain control compared with opiates.27 A smaller randomized controlled trial of patients in the emergency department demonstrated that biliary pain control was similar between ketorolac and butorphanol.28 Compared with nonsteroidal anti-inflammatory drugs, opiates have more adverse effects and may also cause painful sphincter of Oddi spasms.27,28 A 2021 randomized controlled trial evaluated the effectiveness of intravenous lidocaine (100 mg) vs. intravenous morphine (5 mg), demonstrating that lidocaine had faster pain relief with no difference in overall pain reduction.29 Although this study did not report any adverse effects, intravenous lidocaine may be associated with negative inotropic effects and potentiation of arrythmias.
What Are the Best Management Strategies for Patients With Asymptomatic Gallstones?
Incidental or asymptomatic gallstones typically do not warrant further medical intervention. Most of these patients remain asymptomatic; those who develop symptoms rarely experience complications or require surgery.
EVIDENCE SUMMARY
Approximately 80% of U.S. patients with gallstones are asymptomatic.2,15 In a prospective trial of 135 patients with asymptomatic gallstone disease followed for an average of 58 months, only 10% developed biliary symptoms, and 7% needed surgery.30 Gallstone regression is possible; a 24-year follow-up study of patients with asymptomatic gallstones found that only 28% still had gallstones on ultrasonography, whereas only 6% required cholecystectomy.31 An estimated 1% to 2% of those with asymptomatic or incidentally discovered gallstones develop symptoms or complications within a given year.32
Prophylactic cholecystectomy in asymptomatic individuals is usually not performed because of complication rates, surgery risks, and health care costs.32,33 Because of a greater risk for subsequent gallstone formation and complications, prophylactic cholecystectomy may be considered in specific populations, including patients with sickle cell anemia, hereditary spherocytosis, anticipated organ transplant, neuroendocrine tumors, and gallstones larger than 3 cm.1,5,34–36
What Is the Utility of Ursodeoxycholic Acid or Chenodeoxycholic Acid in Gallstone Disease?
Ursodeoxycholic and chenodeoxycholic acids have limited roles in treating gallstone disease, but they can be nonsurgical alternatives for selected patients. Ursodeoxycholic acid prophylaxis is recommended for 6 months after bariatric surgery.
EVIDENCE SUMMARY
Ursodeoxycholic acid (i.e., ursodiol) and chenodeoxycholic acid are oral medications that decrease the hepatic secretion of bile acid; this therapy can promote the gradual dissolution of cholesterol gallstones.37 Oral dissolution therapy should be reserved for patients with symptomatic gallstones who are high-risk surgical candidates or do not wish to undergo surgery. Ursodeoxycholic acid improves pain from gallstones and results in a stone dissolution rate (defined as percentage of gallstone volume reduction) of up to 60%.38–40
Oral dissolution therapy reduces stone burden, but it is less effective in completely eradicating all stones. One study demonstrated that dissolution rates were 47% after 6 months of taking ursodeoxycholic acid and 59% after 12 months; however, complete stone dissolution after 24 months was only 28%.38 One small study showed that 11 years after dissolution therapy, the stone recurrence rate was 49%.41 Ursodeoxycholic acid and chenodeoxycholic acid can be combined, and a meta-analysis evaluating 6 months of combination therapy found that gallstone dissolution rate was 63%.39
Patients who have rapid weight loss after bariatric surgery are at high risk of gallstone formation. These patients should be treated with ursodeoxycholic acid for approximately 6 months after surgery to reduce the risk of gallstone formation (NNT = 5), symptomatic gallstones (NNT = 14), and cholecystectomy (NNT = 18).42,43
What Are Common Complications After Cholecystectomy?
Immediate postoperative complications of laparoscopic cholecystectomy include intra-abdominal bleeding, biliary leak, or a retained gallstone. Postcholecystectomy syndrome encompasses a variety of gastrointestinal symptoms that occur after the procedure.
EVIDENCE SUMMARY
Cholecystectomy is the most common treatment for symptomatic gallstone disease, with approximately 750,000 performed (primarily laparoscopically) each year in the United States.44 Acute postoperative complications include abdominal wall or intra-abdominal bleeding (3.6%), bile leaks (0.4% to 1.9%), surgical wound infections (0.9%), and incisional hernias (0.4%).44,45 The incidence of retained gallstones is estimated to be between 1% and 5%.44
Postcholecystectomy syndrome occurs in 5% to 10% of patients and includes a constellation of gastrointestinal symptoms (e.g., abdominal pain, bloating, diarrhea, dyspepsia, flatulence).46 A systematic review of patients who underwent cholecystectomy found that 13% developed postcholecystectomy diarrhea.47 This condition is thought to be caused by excess bile acid production, likely improves over time, and can be treated with cholestyramine.48
This article updates previous articles on this topic by Abraham, et al.1; Bellows, et al.49; and Ahmed, et al.50
Data Sources: A PubMed search was performed for meta-analyses, randomized controlled trials, systematic reviews, and clinical reviews. Key search terms were gallstone, gallbladder, cholelithiasis, biliary colic, cholecystitis, choledocholithiasis, gallstone pancreatitis, risk factors, imaging, ultrasound, dissolution, and postcholecystectomy. The Cochrane database, JAMA Evidence, ACCESSSS Smart Search, and Essential Evidence Plus were also reviewed. Studies were reviewed and included that used the patient category of sex, but the studies did not define how this category was assigned. Search dates: May 2023 and April 29, 2024.
The authors acknowledge and thank Dr. Justin Anderson, The Ohio State University Wexner Medical Center, Columbus, Ohio, for helping with the initial planning and literature review for this article.
