The major salivary glands are the paired parotid, submandibular, and sublingual glands. Salivary gland disorders can affect the glandular tissue or its excretory system. The parotid glands are the largest and produce aqueous serous secretions that are less immunogenic. They are more susceptible to infections and neoplasms. The submandibular glands produce mucinous secretions that are high in calcium and phosphate salts through a long submandibular duct that flows against gravity. The submandibular glands are responsible for more than 80% of salivary stones. Sialadenitis can be acute or chronic and caused by bacterial, viral, and obstructive etiologies; the most common bacteria is Staphylococcus aureus. The most common viral etiologies in children are mumps (globally) and juvenile recurrent parotitis (in vaccinated populations). Sialadenosis is a chronic asymptomatic enlargement of the salivary glands due to systemic disease. Sialolithiasis causes up to 50% of salivary gland disorders. It is associated with salivary stasis and inflammation caused by dehydration, malnutrition, medications, or chronic illness. Obstruction is also caused by trauma, stenosis, and mucoceles. Neoplasms are rare and typically benign, but they warrant referral and imaging with ultrasonography, computed tomography, or magnetic resonance sialography. Most disorders are managed with conservative measures by treating the underlying etiology, optimizing predisposing factors, controlling pain, and increasing salivary flow with sialagogues, hydration, massage, warm compresses, oral hygiene, and medication adjustment. Sialendoscopy is a gland-sparing technique that can treat obstructive and nonobstructive disorders. (Am Fam Physician. 2024;109(6):550-559. Copyright © 2024 American Academy of Family Physicians.)
Salivary gland disorders can affect the glandular tissue or its excretory system. This article presents a brief evidence-based review of diagnosis and treatment of the multiple etiologies of these disorders.
SORT: KEY RECOMMENDATIONS FOR PRACTICE
| Clinical recommendations | Evidence rating | Comments |
|---|---|---|
| Sialagogues are part of the initial conservative management of obstructive sialadenitis, in addition to massage, heat, and hydration.11,12,51 | C | One systematic review demonstrating malic and citric acid improved xerostomia symptoms, and expert opinion |
| Sialendoscopy is safe and effective for pain relief and diagnosis in patients with chronic obstructive sialadenitis.33,44,45,59,60 | B | Two small retrospective cohort studies, one small cross-sectional study, and expert opinion; one small retrospective study reported that success depends on stone size and location |
| If salivary gland neoplasm is clinically suspected, imaging of the neck and primary site should be performed with ultrasonography, computed tomography with intravenous contrast, or magnetic resonance imaging.8 | C | Expert consensus guideline demonstrating improved tumor characterization, improved pathologic diagnosis through biopsy guidance, and improved operative planning |
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to https://www.aafp.org/afpsort.
Epidemiology
- Sialolithiasis is the most common cause of salivary gland swelling and accounts for up to 50% of all major salivary gland disease. It has a lifetime prevalence of 0.45%.1–3
- Acute suppurative sialadenitis is a rare but serious infection that accounts for 0.02% of all hospitalizations and has a mortality rate of up to 40%.4,5
- The most common viral etiologies in children are mumps (globally) and juvenile recurrent parotitis (in vaccinated populations). The peak incidence occurs between 3 and 6 years of age.6,7
- Salivary gland malignancies account for less than 1% to 6% of head and neck cancers and occur most commonly in the parotid glands.7–10
Anatomy
- The major salivary glands are the paired parotid, submandibular, and sublingual glands; there are also minor glands that line the oropharynx. Each gland secretes saliva to the oropharynx through a duct system. Saliva aids in digestion, lubrication, neutralization of bacterial acid, and protection of the oral mucosa11 (Figure 1).
- Disorders of the salivary glands affect the glandular tissue or its excretory system5 (Table 11,2,5–7,9,11–22 ). Predisposing conditions and medications are listed in Table 2.11,12,23
FIGURE 1.
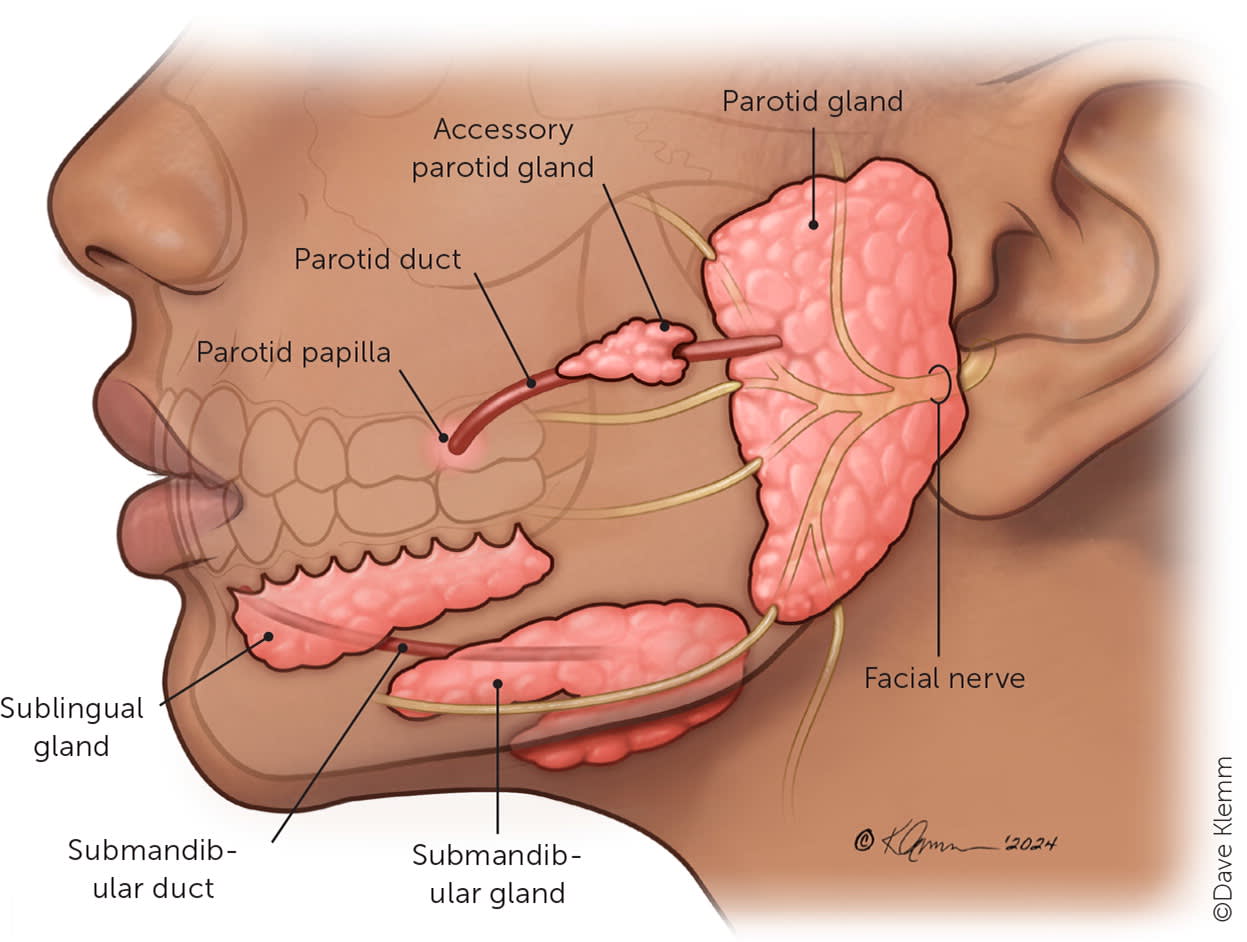
Salivary gland anatomy.
TABLE 1. Pathophysiology and Clinical Presentation of Salivary Gland Disorders
| Disorders | Pathophysiology | Clinical presentation |
|---|---|---|
| Glandular tissue | ||
| Acute suppurative sialadenitis | Inflammation of the salivary gland, typically from bacterial retrograde travel through the salivary duct; decreased oral intake, poor oral hygiene, and systemic illness causing salivary stasis allows for bacterial migration into glandular tissue; the aqueous serous secretions of the parotid glands are less immunogenic, and the glands are more commonly affected | Acute, unilateral pain, inflammation, fever, and erythema of the affected gland; purulence from the affected duct may be seen on examination |
| Nonsuppurative sialadenitis | Viral infections including mumps virus, influenza A, SARS-CoV-2, Epstein-Barr virus, herpes simplex virus, parainfluenza, adenovirus, and HIV cause generalized inflammation of the glandular tissue | Bilateral symmetrical parotid gland edema and pain; often accompanied by a prodrome of flulike illness; some features are specific to the virus (e.g., mumps virus infection is associated with epididymo-orchitis; HIV infection is associated with parotid gland lymphoepithelial cysts) |
| Systemic autoimmune disorders, such as Sjögren syndrome and immunoglobulin G4-related disease, result in immune-mediated and fibroinflammatory tissue damage | Presentation is specific to each disease but commonly includes symmetrical bilateral salivary gland edema and pain; unique features include xerostomia in Sjögren syndrome; diffuse or localized swelling in multiple organs occurs with immunoglobulin G4-related disease | |
| Posttreatment sialadenitis can occur as a complication of radiation, radioactive iodine, or anesthesia | Edema of the affected gland, taste alteration, xerostomia, and salivary gland hypofunction; variable onset of days to months posttreatment | |
| Nonsuppurative sialadenitis | Pneumoparotitis occurs when air within the salivary gland ductal system results in inflammation; an increase in intraoral pressure causes insufflation of the parotid duct; mechanisms include positive pressure ventilation, dental instrumentation, use of wind instruments | Painful or nontender, recurrent, unilateral or bilateral swelling of the parotid glands; crepitus on palpation and frothy saliva expression from the parotid duct |
| Sialadenosis | Excessive hypertrophy of the acinar component of the gland caused by autonomic neuropathy; typically associated with alcoholism, diabetes mellitus, bulimia nervosa, and malnutrition; the gland has no other underlying abnormalities | Chronic, bilateral, asymptomatic hypertrophy of salivary glands (typically parotid glands); swelling is symmetrical and persistent |
| Juvenile recurrent parotitis | Unknown etiology and pathophysiology | Recurrent episodes of unilateral parotitis (occasionally bilateral) that last up to a week and may resolve with puberty; episodes are characterized by parotid gland swelling, pain, malaise, and fever |
| Neoplasm | Pleomorphic adenoma is the most common benign salivary gland neoplasm (70% of all salivary gland tumors); mucoepidermoid carcinoma is the most common malignant neoplasm of the salivary glands; both are most commonly located in the parotid glands | Painless, slow-growing mass in the gland; patients may report pressure sensation and have alarm symptom findings (Table 3) |
| Excretory system | ||
| Obstructive sialadenitis | Salivary stasis and decreased flow from obstruction of excretory duct, resulting in inflammation of affected gland and progressive acinar destruction and fibrous replacement; causes include salivary stones, mass effect, strictures, scarring, and foreign bodies | Chronic, recurrent episodes of pain, inflammation, associated with eating |
| Sialolithiasis | Submandibular glands produce mucinous secretions that are higher in calcium and phosphate salts and cause > 80% of salivary stones; the submandibular duct has a long course and flows against gravity, which contributes to salivary stasis A nidus of complex glycoproteins develops, which leads to further salivary stasis and allows for the precipitation of salts into the glycoprotein matrix | Recurrent episodes of periprandial pain and edema of the affected gland; symptoms can have varying periods of remission; rarely, they are asymptomatic |
| Cysts | Mucoceles are mucin-filled cysts that develop after minor trauma to an excretory duct of a minor salivary gland | Fluid-filled fluctuant mass confined to the floor of the mouth |
| Neoplasm | Some neoplasms are specific to the excretory system, such as intraductal carcinoma and salivary duct carcinoma; tumors can cause obstructive salivary gland disorders through mass effect | Painless, slow-growing mass in the gland, may have alarm symptom findings (Table 3) |
TABLE 2. Risk Factors for Salivary Gland Disorders
| Systemic conditions | ||||
| Alcoholism Amyloidosis Cachexia Cirrhosis | Cushing syndrome Cystic fibrosis Dehydration | Diabetes mellitus Eating disorders Hypothyroidism | Immunoglobulin G4-related disease Malnutrition Obesity | Sarcoidosis Sjögren syndrome Toxoplasmosis |
| Medications* | ||||
| Anticholinergics Atropine Hyoscyamine Scopolamine Tiotropium (Spiriva) Antidepressants Amitriptyline Bupropion Citalopram Duloxetine (Cymbalta) Escitalopram Fluoxetine Imipramine Nortriptyline Paroxetine Sertraline Venlafaxine | Antiepileptics Gabapentin Pregabalin (Lyrica) Valproic acid Antihistamines Cetirizine Diphenhydramine Doxylamine Fexofenadine Hydroxyzine Loratadine Anti-insomnia Zolpidem Anti-obesity Orlistat Phentermine | Antiparkinsonism Carbidopa/levodopa Antipsychotics Aripiprazole Chlorpromazine Clozapine Haloperidol Lithium Olanzapine (Zyprexa) Quetiapine Risperidone Ziprasidone Benzodiazepines Alprazolam Clonazepam Diazepam Lorazepam | Cardiovascular Atenolol Clonidine Furosemide Lisinopril Methyldopa Prazosin Propranolol Tolvaptan Verapamil Genitourinary Alfuzosin (Uroxatral) Oxybutynin Terazosin Tolterodine | Musculoskeletal Baclofen Cyclobenzaprine Tizanidine (Zanaflex) Opioids Buprenorphine Butorphanol Fentanyl Morphine Tramadol Osteoporosis Alendronate Sympathomimetics Dexmethylphenidate (Focalin) Lisdexamfetamine (Vyvanse) Methylphenidate |
*—Listed medications are reported to cause xerostomia, salivary gland hypofunction, or sialorrhea with higher and moderate levels of evidence.
Diagnosis
INFLAMMATORY (SUPPURATIVE SIALADENITIS)
- Suppurative sialadenitis occurs most commonly in the parotid glands, ascending through the parotid duct. Pre-disposing factors include decreased salivary output secondary to dehydration, obstruction, systemic illness, or certain medications. The most common bacterial cause is Staphylococcus aureus.11–13,24
- Presentation includes unilateral pain and inflammation overlying the affected gland. This can progress to fever, trismus, and abscess formation. Purulence can be expressed or visible from the parotid duct11,13,25 (Figure 213 ).
- Computed tomography is the preferred imaging method, followed by ultrasonography.5
FIGURE 2.
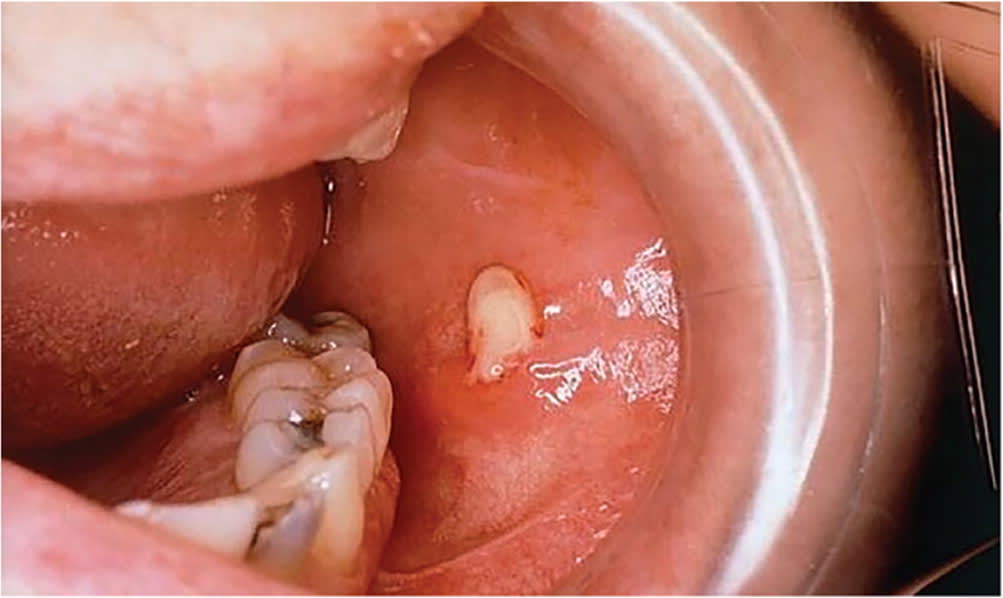
Intraoral view of purulence emanating from the parotid duct orifice in a patient with acute suppurative parotitis.
Reprinted with permission from Wilson KF, Meier JD, Ward PD. Salivary gland disorders. Am Fam Physician. 2014;89(11):884.
INFLAMMATORY (NONSUPPURATIVE SIALADENITIS)
- Viral etiologies include mumps virus, HIV, human herpesvirus (e.g., Epstein-Barr virus), influenza A virus, human parainf luenza virus, coxsackievirus, cytomegalovirus, and SARS-CoV-2.26–28
- Viral sialadenitis presents with acute bilateral, tender, and diffuse edema of the salivary glands.11,25
- Bilateral benign lymphoepithelial cysts of the parotid glands are a classic manifestation of HIV infection, and ultrasonography should be performed if they are clinically suspected.14,29
- In children who have received the mumps vaccination, recurrent juvenile parotitis is the most common parotid disease. Its etiology is unknown. Patients experience one to five episodes per year of mostly unilateral parotitis with malaise and fever, which may last up to a week.6
- Posttreatment sialadenitis occurs as a complication of radiation, radioactive iodine, or anesthesia. Symptoms occur within days to months. It presents with edema of the gland, taste alteration, xerostomia, and salivary gland hypofunction.15,16
- Autoimmune diseases commonly manifest with chronic salivary gland disorders and multisystem involvement. Immunoglobulin G4-related disease, Sjögren syndrome, and systemic lupus erythematosus may present with salivary gland edema or xerostomia.30 Presentation and evaluation are unique to each disease17,18,25 (Figure 311,13,24,25,31–34 ).
FIGURE 3.
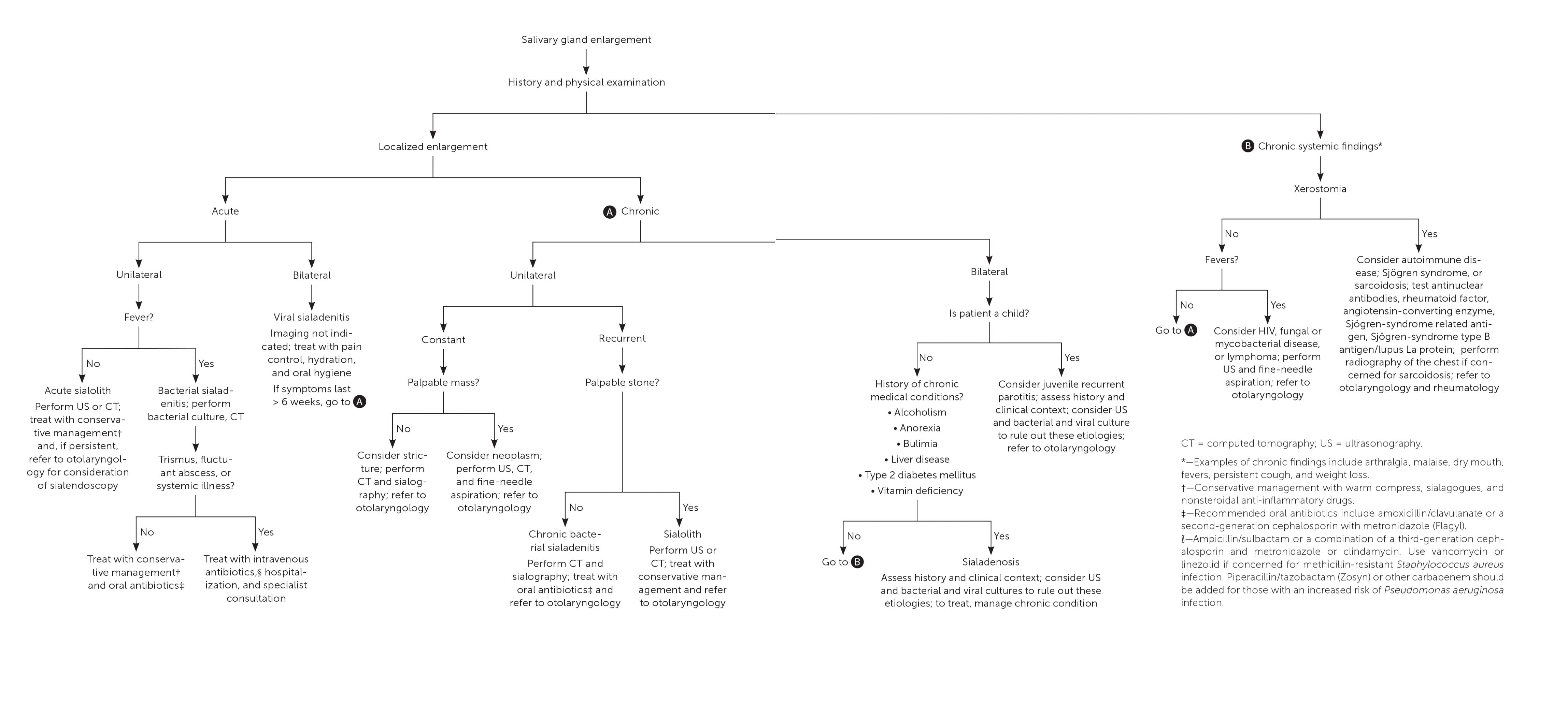
Evaluation and management of salivary gland disorders.
NONINFLAMMATORY
- Sialadenosis is a bilateral, asymptomatic enlargement of the salivary glands. Etiologies include chronic systemic diseases such as eating disorders, thyroid dysfunction, alcoholism, liver disease, and diabetes mellitus.31
- Diagnosis is based on the exclusion of inflammatory, obstructive, or malignant processes using imaging or fine-needle aspiration.31
OBSTRUCTIVE
- Obstructive sialadenitis is most commonly caused by sialolithiasis. Other causes include orifice impaction (e.g., foreign body), trauma, and stenosis. The presentation is similar to nonsuppurative sialadenitis.11
- Sialolithiasis presents with recurrent episodes of periprandial pain and swelling of the salivary gland with periods of remission. On examination, a sialolith may be palpable, but symptoms of infection are absent.12,13
- Sialolith formation is associated with factors contributing to salivary stasis and inflammation (e.g., dehydration, malnutrition, medications).11,35
- The sensitivity and specificity of ultrasonography for sialolithiasis range from 65% to 95% and 80% to 97%, respectively (positive likelihood ratio [LR+] = 7.3; negative likelihood ratio [LR−] = 0.22, based on midpoints of the ranges).36–38 Contrast-enhanced computed tomography has a sensitivity and specificity of 96% to 98% and 88% to 100%, respectively (LR+ = 16; LR− = 0.03, based on midpoints of the ranges).36,39
- Mucoceles are mucin-filled cysts that present on the lower lip. They are caused by a ruptured duct of a minor salivary gland secondary to biting or other trauma.11,35 Diagnosis is based on physical examination.19
- Ranulas are mucoceles of the oropharyngeal floor. Plunging ranulas extend to, or beyond, the mylohyoid muscle. A unilateral cyst on the floor of the mouth may be observed. The effectiveness of ultrasonography is comparable to computed tomography when correlated with surgical findings (sensitivity of 90% to 97%).11,25,40,41
NEOPLASTIC
- Salivary neoplasms can present with alarm symptoms (Table 31,13,42 ). A firm, painless mass accompanied by lymph-adenopathy may be seen. A cranial nerve examination should be performed to assess for nerve palsy due to a mass effect.42
- Imaging methods include ultrasonography, computed tomography, and magnetic resonance sialography (Table 41,5,11,34,36–38,43–48 ). Fine-needle aspiration has a sensitivity of 80% (95% CI, 0.76 to 0.83).8,49
TABLE 3. Alarm Symptoms and Signs Suggestive of Salivary Gland Malignancy
| History |
| Intermittent and increasing pain |
| Paresthesia of surrounding sensory nerve |
| Previous head and neck radiation |
| Previous skin or salivary gland neoplasm |
| Rapid increase in size of a lump |
| Sjögren syndrome |
| Clinical signs |
| Cervical lymphadenopathy |
| Facial nerve weakness |
| Fixation of mass to underlying tissue |
| Overlying skin or mucosal changes (e.g., ulceration, induration) |
TABLE 4. Indications for Imaging With Salivary Gland Disorders
| Imaging method | Clinical scenario | Indication |
|---|---|---|
| Ultrasonography | Quick, cost-efficient, safe, and able to delineate benign vs. malignant features, especially superficial lesions; considered first-line; preferred test in children Difficult to differentiate some sialolithiasis from stenosis or glandular calcifications; deeper portions of the parotid gland are difficult to image User-dependent; sonographer should be experienced in head and neck imaging | For salivary stones: sensitivity of 65% to 95%, specificity of 80% to 97%, LR+ = 7.3, LR− = 0.22 based on midpoints of the ranges |
| Computed tomography | Preferred for acute sialadenitis May be limited by extensive dental artifacts | For salivary stones: sensitivity of 96% to 98%, specificity of 88% to 100%, LR+ = 16, LR− = 0.03 based on midpoints of the ranges |
| Sialendoscopy | Allows for direct visualization and intervention of salivary ducts and obstructions; effective in long-term management of chronic sialadenitis due to obstructions | Successful stone retrieval rate of 86% (95% CI, 83% to 89%)43 Success rates vary widely according to disease, affected glands, number of stones, and site of ductal abnormality |
| Conventional sialography | Evaluates the overall ductal system of salivary glands by injecting contrast media into the parotid and submandibular ducts; not used in the era of computed tomography and magnetic resonance sialography | – |
| Magnetic resonance sialography | Does not require intraductal injection of contrast media; evaluates the overall ductal system of the salivary glands; limited by longer time requirements | Comparable to conventional sialography for detection of obstructions, strictures, and stenosis |
LR+ = positive likelihood ratio; LR− = negative likelihood ratio.
Treatment
INFLAMMATORY (SUPPURATIVE SIALADENITIS)
- Management of acute suppurative sialadenitis starts with empiric antibiotics, treating the underlying etiology, and optimizing predisposing factors. Salivary flow is increased with sialagogues (e.g., vitamin C lozenges), hydration, massage, warm compresses, oral hygiene, and adjustment of medications.11,13,25,50 Citric acid and malic acid (found in lemons, limes, apples, and grapes) also stimulate salivary flow.51
- Patients with systemic signs of illness should receive empiric intravenous antibiotics followed by oral step-down therapy. Oral antibiotics may be appropriate in the absence of systemic illness or for mild cases (Table 512,32,50,52 ).
- Abscesses should be drained, and purulent material should be cultured to guide treatment.4,12,50
TABLE 5. Recommended Antibiotics for Acute Suppurative Parotitis*
| Intravenous | Oral | |
|---|---|---|
| First-line therapies† | Ampicillin/sulbactam, 3 g every 6 hours or Ceftriaxone, 1 to 2 g daily (or other third-generation cephalosporin) and Metronidazole (Flagyl), 500 mg every 8 hours or clindamycin, 600 to 900 mg every 8 hours | Amoxicillin/clavulanate, 875 to 125 mg every 12 hours or Cefuroxime, 500 mg every 12 hours (or a macrolide for penicillin allergies) and Metronidazole, 500 mg every 8 hours |
| Patients with risk factors for methicillin-resistant Staphylococcus aureus‡ | Vancomycin, 20 to 35 mg per kg loading dose, then 15 mg per kg every 12 hours (maximum: 3 g per dose)§ or Linezolid, 600 mg every 12 hours | Not applicable |
| Patients with risk factors for Pseudomonas aeruginosa|| | Piperacillin/tazobactam (Zosyn), 3.375 g every 6 hours or 4.5 g every 8 hours or Meropenem, 1 g every 8 hours (or other carbapenem) | Not applicable |
*—Antibiotic dosing information provided from Lexicomp Database and expert opinion.
†—Recommended first-line agents are based on expert opinion, case reports, and microbiology. Pathogens targeted include Staphylococcus aureus, Streptococcus viridians, anaerobes, and gram-negative organisms such as Escherichia coli. Rare organisms include Haemophilus influenzae and Klebsiella pneumoniae.
‡—Includes recent hospitalization or antibiotics, hemodialysis, diabetes mellitus, and residence in a long-term care facility.
§—These antibiotics should substitute for first-line therapies if used.
||—Includes immunocompromised patients or residence in a long-term care facility.
INFLAMMATORY (NONSUPPURATIVE SIALADENITIS)
- Viral infections are self-limited and treated with supportive care.11
- The measles, mumps, and rubella vaccine is safe and effective, although outbreaks in vaccinated populations have increased. The Centers for Disease Control and Prevention recommends a third dose of the vaccine for those at risk, as determined by public health authorities, during outbreaks.14,53–55
- Chronic sialadenitis is managed conservatively and by treating the underlying cause.11,12
- Surgical excision is reserved for refractory cases; it carries the risk of facial nerve palsy and fistula.31,42,56
- Recurrent juvenile parotitis is treated with supportive care and exclusion of other diseases. It may resolve with puberty. Children with symptoms that do not improve with conservative measures may benefit from sialendoscopy.6,57
- Posttreatment sialadenitis is treated with supportive care and exclusion of other diseases. There is limited evidence for prevention of salivary dysfunction.15
NONINFLAMMATORY
- Management of sialadenosis comprises treating the underlying cause and adjusting medications.11 Conservative measures include decreasing swelling by stimulating salivary flow. Moderate evidence supports use of cevimeline (Evoxac) and pilocarpine for xerostomia, but they can be associated with significant adverse effects. Surgical intervention may be indicated if sialomegaly causes distress.11,31,51,58
OBSTRUCTIVE
- Obstructive sialadenitis is managed conservatively. Imaging is recommended if there is no improvement within 48 hours.5
- Management of sialolithiasis begins with conservative measures (i.e., gentle massage, moist heat, hydration, and sialagogues). Nonsteroidal anti-inflammatory drugs can reduce pain. Surgical removal is the mainstay of therapy.12,13
- Sialendoscopy is a gland-sparing technique that can relieve symptoms of chronic obstructive salivary gland disorders.33,44,45,59,60
- Further interventions include extracorporeal shockwave lithotripsy, laser lithotripsy, and transoral robotic surgery.42,61
- Mucoceles are managed with observation but are likely to recur. The primary treatment is surgical excision, with newer therapies being introduced (e.g., intralesional sclerosing agents, laser ablation).7,19
- Ranulas can be managed similarly to mucoceles, but plunging ranulas require surgical excision.19,62
NEOPLASTIC
- Up to 70% of salivary gland neoplasms are benign, but referral is still indicated. The most common benign tumor, pleomorphic adenoma, can become malignant.1,20
- Imaging with ultrasonography, computed tomography, or magnetic resonance imaging of the neck, in addition to the primary site, should be performed. Treatment may include surgical resection and radiotherapy.8
This article updates a previous article on this topic by Wilson, et al.13
Data Sources: A PubMed search was completed using the key terms parotitis, sialadenitis, salivary glands, sialoliths, sialendoscopy, sialography, imaging salivary glands, parotid gland, submandibular gland, sublingual gland, mumps outbreak, mumps vaccination, Sjögren syndrome, IgG4-related disease, salivary stimulation, sialadenosis, xerostomia, pilocarpine, suppurative sialadenitis, viral sialadenitis, radiation-induced sialadenitis, sialithiasis, mucocele, ranula, salivary gland tumor, and salivary gland malignancy. Also searched were the Cochrane database, Trip Database, and Essential Evidence Plus. Search dates: May, June, August, November, and December 2023 and April 2024.
The opinions and assertions contained herein are the private views of the authors and are not to be construed as official or as reflecting the views of the U.S. Department of Defense, Uniformed Services University of the Health Sciences, U.S. Air Force, or U.S. government.
