CASE SCENARIO
As someone who takes pride in maintaining meaningful patient-clinician relationships, I was upset to learn that a 38-year-old Black patient, whom I have seen multiple times in my clinic, requested a referral for contraception management. She has one living child, a previous pregnancy termination, and a history of obesity, hypertension, and depression. I have extensive experience in contraceptive management and believe that assisting patients with sexual and reproductive health care is a priority in primary care.
In a previous visit, I had suggested an intrauterine device as a potential contraception method, but she seemed ambivalent about the recommendation at the time. On reflection, I did not adequately discuss her sexual and reproductive health goals and contraceptive method preferences. I also did not consider her experiences of discrimination in health care, history of sexual trauma, or other issues that may impede her ability to trust clinicians, especially regarding sensitive topics.
As a male physician from a different cultural background, could I have unintentionally created a perception of a hidden agenda? How can I improve my approach to sexual and reproductive health care to understand patients' experiences and better meet their needs?
COMMENTARY
The complex dynamics of patient encounters such as this scenario are common across care settings. Implicit or explicit biases, subtle pressures, or even coercion on the part of the clinician can profoundly influence contraception counseling sessions.1 Clinicians are sometimes unaware of power dynamics that influence the visit and may inadvertently evoke patient perceptions of coercion and an unsafe health care environment.2
Many patients or those close to them have encountered or heard first-hand accounts of government-sponsored forced sterilizations, experimentation with contraceptives without consent, eugenics, and other ethnicity- or race-based mistreatment in sexual and reproductive health care. Such experiences can have a lasting influence and be reminiscent of some recent unbalanced sexual and reproductive health care initiatives, including provision of select no-cost options (e.g., long-acting reversible contraception) for those with limited resources who cannot afford their preferred method. This background converges with racism, sexual violence, and unsafe health care environments to enhance mistrust and vigilance in health care settings even when health care professionals are well-intentioned.1,3 Medical mistrust is often a part of the individual and collective consciousness in communities of color.4 Providing health care and conducting research, especially in sensitive areas such as contraceptive care, necessitates ongoing calibration with current cultural and societal contexts.5
To best serve patients, clinicians should strive to understand the effect of mistreatment regarding sexual and reproductive health, conceptually, for those who have been historically underserved, marginalized, and excluded.1 This population includes people of color, immigrants, and people who have disabilities, lower income, younger age, sexual or gender-diverse identities, or substance use disorder. It also includes those whose sexual and reproductive health care concerns have been devalued. The goal is to eliminate the occurrence and sequelae of biases and barriers, including those that are systemic and structural, contributing to mistreatment.1,6,7
The American College of Obstetricians and Gynecologists and the American Public Health Association explicitly recommend a patient-centered, reproductive justice–based contraception counseling framework1,8 (Table 11,2,6,8,9); yet, many people are not using their preferred method.10 To achieve this goal, the clinician should focus on ensuring universal access to the widest range of contraceptives, including, but not limited to, long-acting reversible contraception.6,8,9 Well-intentioned efforts to increase access to long-acting reversible contraception, without deliberate planning, could be misconstrued as an effort to “push” this contraception on an individual patient, causing unintended harm. Instead, the clinician should recognize that some people may prioritize other factors such as attaining regular, tolerable menses over the most effective option in preventing pregnancy because unintended pregnancy is not always viewed as a negative outcome by patients.6,8,9
TABLE 1. Approaches to Contraception Counseling
| Counseling approach | Features | Disadvantages |
|---|---|---|
| Patient-centered approach* | Focuses on achieving a person's described sexual and reproductive health goals, primarily through shared decision-making (with flexibility to switch to another approach if requested by the patient), based on the person's values, lived experiences, and preferences | May require additional clinician thoughtfulness and reflection, taking more time in clinical encounters |
| Tiered-effectiveness model | Encourages clinicians to prioritize discussions around the most effective options for pregnancy prevention | Does not intrinsically elucidate the range of patient goals Can be perceived as coercive Clinicians may inadvertently conflate population-level indicators such as contraceptive method uptake and unintended pregnancy rates with an individual patient's needs |
| Menu-based approach | Clinicians provide education but limit influence based on order of method presentation to avoid coercion, improve autonomy, and improve counseling efficiency | Many patients desire clinician input when making decisions around contraception Decision tools structured in alphabetical order may be difficult for some people to follow |
| Physician-directed approach | Clinicians recommend specific methods based on perceived patient benefit; common in the care of adolescents | Does not intrinsically elucidate the range of patient goals Can be perceived as coercive |
*—Preferred method.
Practical Approach
Patients value comprehensive counseling, personalized information, autonomy, decision-making support, confidentiality, and positive interpersonal environments when receiving contraceptive counseling.11,12 For example, adolescents may particularly value social context such as friends' experiences.12 A systematic review and meta-analysis not specific to any racial or ethnic groups found that enhanced counseling interventions (e.g., with shared decision-making components) increased contraceptive use by 39% 3 to 6 months later (risk ratio = 1.39; 95% CI, 1.16 to 1.72; 10 trials; n = 5,239) compared with usual care.5 Improving the patient's experience of care can increase continuation of and satisfaction with contraception, optimize method use, and reduce unintended pregnancy.2,13,14
Setting the Stage. At any clinical visit, a clinician can ask whether the patient would like to talk about contraception. Alternatively, or in sequence, a clinician can ask whether the patient wants or plans to become pregnant in the next year; One Key Question offers an iterative approach to begin the converstion about pregnancy desires.15 Note that when asked in isolation, questions about pregnancy intention are not particularly sensitive for detecting interest in contraceptive care. With relevant follow-up questions, either approach can identify reproductive health goals, priority for pregnancy prevention (including in the peripartum timeframe), and need for preconception services.16–18 Not everyone desires or can achieve pregnancy, and preferences may be complex; therefore, sensitivity is paramount.2 If contraception counseling is indicated, the clinician should elicit information that would help determine medical eligibility criteria.19
Shared Decision-Making Process. Shared-decision processes begin with questions such as, “Do you have a sense/idea of what is important to you about your method?”20 Such open approaches root the discussion in clear patient-centered terms while avoiding immediate anchoring on specific methods. It also helps clarify the extent to which the patient desires education and feedback.20
For patients who are unsure about their contraceptive method preferences, the clinician can prompt the patient: “Methods differ in how they are used, their effect on periods, how reliable they are in preventing pregnancy, and other ways. Can we talk about your feelings around these factors?”20
A patient-centered visual aid that does not exclusively focus on effectiveness can guide next steps. Ideally, a table or chart organized by patient-centered priority items should clearly display effects on menstrual bleeding, possible adverse effects, noncontraceptive benefits, and other factors patients may find valuable (eFigure A). Alternatives without such organizing principles (e.g., methods listed in alphabetical order) may be difficult for some patients to follow. Bedsider provides an online evidence-based resource that allows individuals to review side-by-side profiles of options. Interactive phone apps are also becoming increasingly available. It is vital for the clinician to understand that if patients have the perception that conversations are influenced by the clinician's method preference or agenda, the patients are at greater risk of method dissatisfaction than those without this perception.13 Cost may also be a leading deciding factor.
eFIGURE A
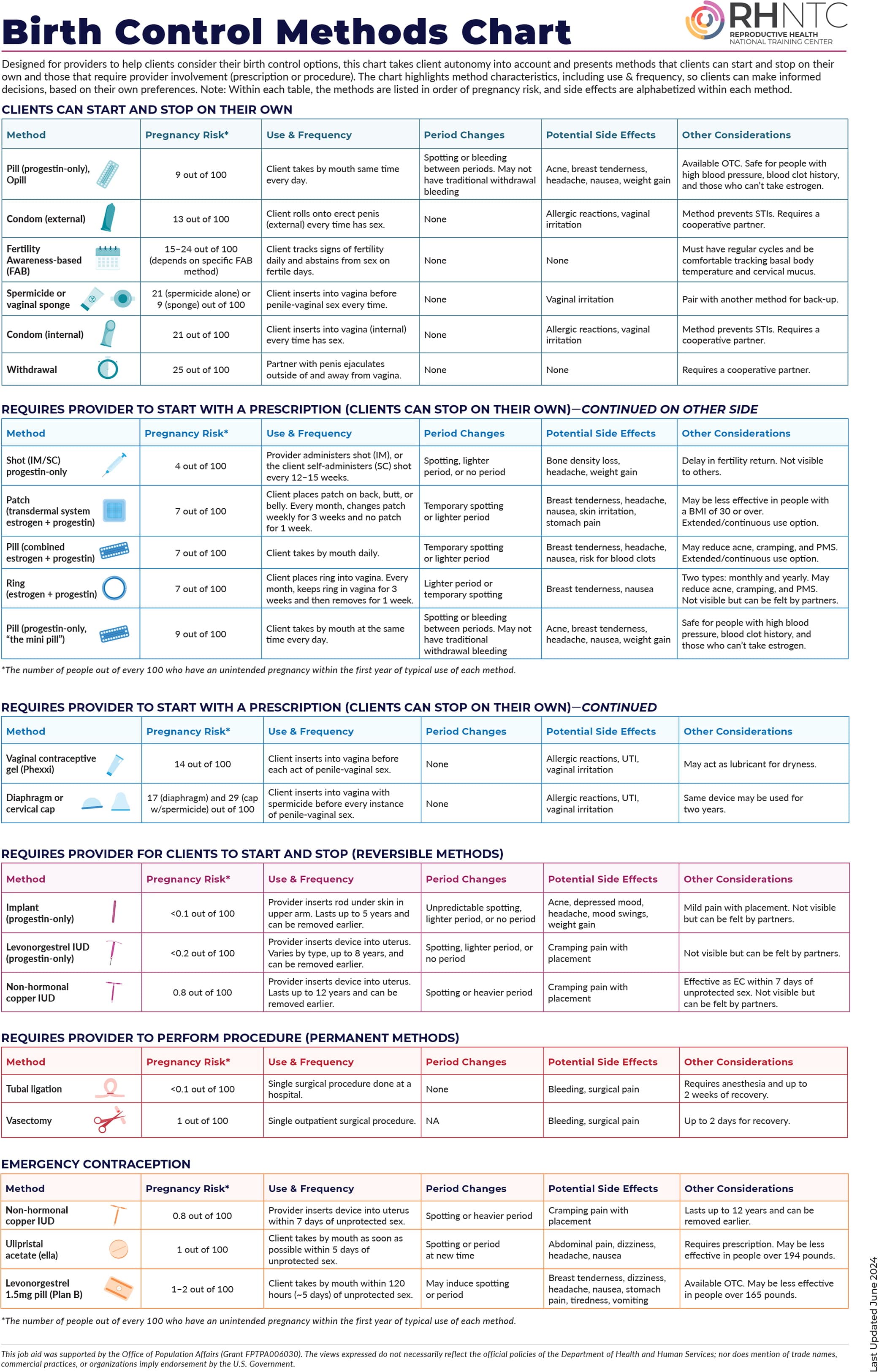
Reprinted with permission from Reproductive Health National Training Center. Birth control methods chart. July 26, 2024. Accessed August 19, 2024. https://rhntc.org/sites/default/files/resources/rhntc_birth_control_methods_chart_7_26_2024.pdf
Patient-centered counseling techniques can prevent or address misconceptions in discussions (Table 220,21). When the patient voices a concern, the clinician can reflectively listen; provide a genuine, empathetic statement; and summarize the concern. It can be helpful to acknowledge that others may have experienced the concern or adverse effect in question. After these validating statements, the clinician can check in with the patient to ensure the concern is understood and offer further clarifying information if needed.20 During these responses, the patient is invited to be the final decision-maker.1
TABLE 2. Patient-Centered Contraceptive Counseling Techniques
| Counseling element | Example statements |
|---|---|
| Initiating the conversation | Do you have a sense/idea of what is important to you about your method? What kind of birth control methods have you considered? |
| Eliciting preferences | Methods differ in how often you take them, how they affect your bleeding, and how effective they are at preventing pregnancy, among other things. Here is a chart that summarizes some of the features of the different methods. Tell me about what is most important to you. Some methods involve taking a pill, getting a shot, applying a patch on your skin, inserting a vaginal ring, timing ovulation, using a barrier, or placing protection under the skin of your arm or in your uterus. Do you have preferences or questions about any of these options? Great, I'll avoid talking about methods that you cannot switch quickly. I appreciate your telling me that you want a method that is easy to remember using. |
| Reflective listening | Thank you for sharing your thoughts about that method and trusting me with that information. That's good to hear. It helps me to provide you with some extra details you may be interested in to make your decision. Thanks for telling me you have already picked a method. Do you have any questions about this or other methods? I just want to make sure you know all the options. |
| Responding to concerns or objections | Absolutely! A lot of people feel more comfortable when they have a regular period. Let's talk about options that generally lead to regular periods, but I want you to know that it is safe if the method you pick reduces menstrual bleeding. It's unfortunate that your friend had mood changes and weight gain when they used that method. This can happen, but it is unlikely overall. If you choose that method, we can quickly make a change at your request. It is true that some people like your friend experience irregular menstrual bleeding with the contraceptive implant, but steps can be taken that may help if that happens. |
| Summing the factors that inform the patient's decision | It sounds like your biggest priorities in choosing a method today are not getting pregnant and not having to remember to take a pill every day or come in for a shot. Is that correct? Based on your goals and the information we talked about, what method do you think would be the right fit for you? |
After the patient selects a method, the clinician should start the method if medically safe.22,23 Then, to optimize satisfaction with and continuation of the chosen method, anticipatory counseling on initiation, use, and potential adverse effects should be provided. Finally, the clinician should ensure that the patient has an extended supply and address any related needs (e.g., sexually transmitted infection testing and prevention). Seamless clinic access, such as virtually or through a patient portal, should be offered to address any immediate questions or concerns about the method as they arise. Follow-up visits can examine factors in the patient's life that might interfere with sexual and reproductive health goals or consistent method use, such as family plans, lifestyles, or noncontraceptive needs.2 To preserve a patient's autonomy, method switching or discontinuation must occur promptly in response to a patient's request.1,2,6
CASE RESOLUTION
In this scenario, the clinician should honor the patient's request for a referral. If the patient-clinician rapport allows for additional discussion, the clinician can sensitively offer, in preparation for the referral consultation, to assist in facilitating any of her personal sexual and reproductive health–related goals and preferences and inquire how he can better serve her ongoing health needs in other areas. Lessons learned about patient-centered care from this interaction could lead to more meaningful and effective future patient-clinician interactions and outcomes for sexual and reproductive health and other services.
The contents of this article are solely the responsibility of the authors and do not necessarily represent the official views of the Uniformed Services University of the Health Sciences, the U.S. Air Force, the U.S. Department of Defense, or the U.S. government.
