Each time we share treatment decision-making with patients, the conversation depends in part on studies applicable to their individual situations. It would be a tremendous help to have the results of these studies translated from the academic literature into understandable summaries that could be applied during a clinic visit.
GP Evidence is a free website hosted by the Nuffield Department of Primary Care Health Sciences, University of Oxford, United Kingdom. Designed primarily for family physicians, it offers readily understandable summaries of the evidence behind treatments for common long-term conditions. Using infographics and clear design, GP Evidence highlights the absolute benefits and harms of interventions (absolute risk reduction, number needed to treat, and absolute chance of harms) alongside supportive, contextualized written content. This information can help with single treatment decisions or when prioritizing treatments. Information is aimed at clinicians rather than patients (in contrast to a patient decision aid). An illustration of its use is presented in the case scenario at the end of this editorial.
Guidelines are an essential part of family medicine practice, but they often obscure the size of benefits and give little information about harms.1 The preponderance of relative risk reduction framing in literature exaggerates treatment benefits. Absolute risk estimates are vital to accurately counsel patients.2 It is difficult for clinicians to stay abreast of the evidence regarding the absolute benefits and harms of every intervention.3
GP Evidence provides useful information to support person-centered care in a way that is both appropriate and flexible for a particular person and context.
User-centered design. Although treatment effect estimates are straightforward mathematically, they can be difficult to interpret.4 Even when the information is understood, there are barriers to its use such as pressure to follow guidelines and quality incentives, challenges of communicating choice and shared decision-making, and time constraints.5 To overcome these barriers, a codesign approach was used for GP Evidence.6 This meant that family physicians and patients had active and early input into website development, involving in-depth interviews, stakeholder work, codesign workshops, iterative user testing, and accessible content design principles.6,7
Evidence sources. To ensure trustworthiness and reliability, and alignment with UK practice, most evidence was drawn from the publicly available high-quality evidence reviews from the National Institute for Health and Care Excellence (NICE). If information was not available from NICE reviews, pragmatic literature searches were conducted, drawing mainly on Cochrane reviews and other high-quality systematic reviews.8 It is important to emphasize that GP Evidence does not attempt to make recommendations. Rather, it presents the evidence underpinning guideline recommendations in a neutral, non-directive way.
A common concern for clinicians is pressure to follow guideline recommendations and meet quality incentives. GP Evidence supplies information to enable truly informed consent about treatment options, supporting clinically appropriate exclusions in the electronic health record.
Applicability to the US setting. This global medical evidence base certainly is applicable for US clinicians, although they may notice that US guidelines have different recommendations. Different baseline risk scores may be more applicable to US populations (eg, the American College of Cardiology/American Heart Association PREVENT calculator or ASCVD score rather than the QRISK score). In these cases, it would be appropriate to use the US estimates in place of the UK equivalents—the calculation of treatment benefits from trials will still be correct. When US guidelines recommend lower thresholds or targets, users will be able to glean a broad estimate of benefits from GP Evidence, although they may need to examine the references of the US guideline to clarify. A US version of GP Evidence could be developed in the future.
Updating. GP Evidence is updated when NICE guidelines or technology appraisals are updated. This ensures that evidence has been subject to rigorous review, but this also means that it takes some time for new evidence to be included.
Evaluation. Focus groups of British general clinicians responded positively to GP Evidence, perceiving it as a usable tool to support their practices. They described hypothetical changes to prescribing intentions and increases in decisional confidence.9 Further evaluation is planned to examine the real-world effect of GP Evidence on decision-making and patient experience.
A vision. Evidence-based medicine has arguably transitioned into what we might call “guideline-directed” medicine. Clinical guidelines have many strengths but also limitations such as discouraging person-centered care and disempowering clinicians.10,11 These problems have been well described over the past three decades, but there have been only isolated (rather than systematic) attempts to fix them.12 We hope GP Evidence is a useful contribution to this endeavor, alongside existing online resources and decision support tools integrated into electronic health records. Clinical guidelines should be accompanied by transparent and usable information to support person-centered care, inform shared decision-making, and empower family physicians and the family medicine specialty.
CASE EXAMPLE
A 64-year-old patient has had a cardiovascular risk assessment that estimates his 10-year risk of cardiovascular events as 15%. Clinical guidelines and local quality incentives recommend prescribing a statin. However, your patient prefers not to take medications in general and is concerned about potential adverse effects.
During the consultation, you go to GP Evidence and locate the section illustrating the evidence for the benefits of statins. A drop-down menu is used to select baseline cardiovascular risk, and an infographic is displayed showing an easily understandable summary of treatment benefits (Figure 1). A separate tab shows absolute risk estimates of adverse effects and harms.
FIGURE 1. GP Evidence example.
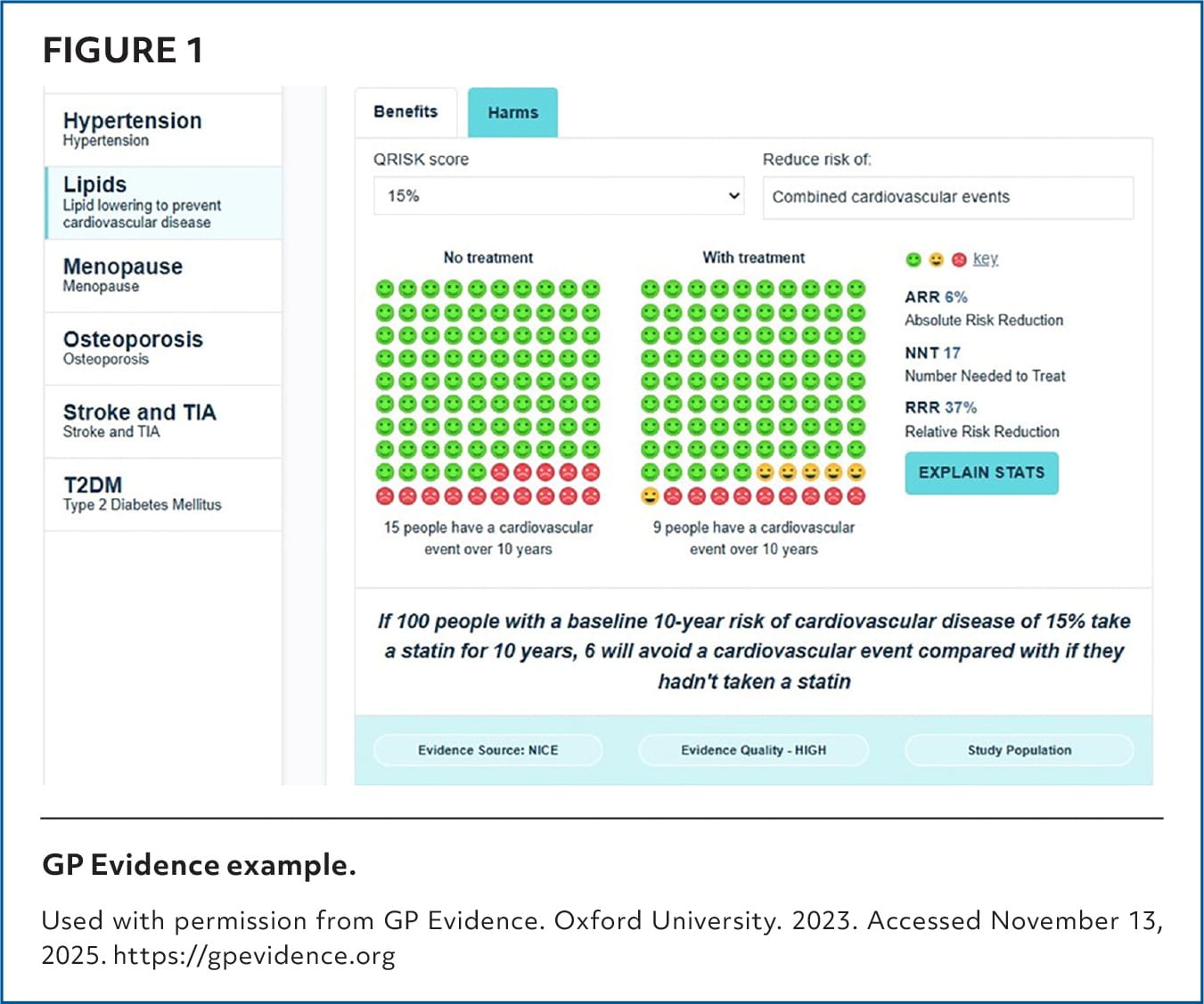
Used with permission from GP Evidence. Oxford University. 2023. Accessed November 13, 2025. https://gpevidence.org
You use this information to frame your conversation with the patient. This may involve showing them the screen, delivering the numbers, and explaining the treatment decision. Some patients want this degree of autonomy. However, it often may be more appropriate for the clinician to have a more qualitative discussion, now empowered by their own improved knowledge of the absolute benefits and harms of treatment. The BRAN (benefits, risks, alternatives, nothing) framework is an effective way to structure these consultations.
Editor’s Note: GP Evidence was developed by Dr. Treadwell and funded by a grant from the UK National Institute for Health and Care Research (NIHR DRF-2018 to 11-ST2 to 021). Intellectual property is held by the University of Oxford. The website is freely available and is not intended to be commercialized. Maintenance of the website is currently undertaken as part of Dr. Treadwell’s academic role, which is funded by the NIHR.
