In 2023, the US Preventive Services Task Force (USPSTF) reaffirmed its 2019 recommendation to prescribe HIV preexposure prophylaxis (PrEP) for adolescents and adults at higher risk of contracting HIV.1 USPSTF recommendations increased clinician adoption and patient use of preventive services.2,3 However, federal reorganization and legal challenges are threatening the USPSTF's autonomy and independence, which could impact provision of PrEP.4,5 Primary care clinicians are critical to delivering preventive care. Federal support for PrEP and primary care prescriptions are both essential for continued progress toward ending the HIV epidemic in the United States.
When taken daily as prescribed, orally or by injection, PrEP reduces the likelihood of acquiring HIV by 96%. Even with suboptimal dosing (ie, two doses per week), the risk reduction remains high at 76%.1 The USPSTF recommendation that physicians prescribe PrEP for patients at increased risk of acquiring HIV eliminated cost-sharing in most insurance plans and contributed to the national decline in HIV prevalence between 2016 and 2020.6
Access to PrEP may vary by geographic disparities and the density of primary care physicians. Areas with higher density were expected to have higher PrEP prescription rates than areas with lower density. The AIDSVu public data resource provided PrEP prescription rates for 2017 and 2023 and the rate of change in prescriptions.7 Primary care physician density was determined using the American Medical Association Physician Masterfile data on practice locations.8
PrEP prescriptions are highest in New England, southern California, and southern Florida. In 2017 and 2023, counties with the highest density of primary care physicians had the highest prescription rates. In 2017, there were approximately 69.2 primary care physicians per 100,000 people in counties in the highest quartile of prescribing, and 57.3 per 100,000 in the lowest quartile. Findings were similar in 2023.
However, there was no correlation between prescription rates increasing from 2017 to 2023 and primary care physician density (Figure 17). Although the largest increases in prescriptions were in Florida, South Carolina, and Arizona, these areas did not have the highest primary care physician density. The rate of PrEP prescriptions increased predominantly in rural and southern states that had low prescribing in 2017, potentially due to destigmatization of PrEP and increased prescribing by health departments, nurse practitioners, and physician assistants.
FIGURE 1.
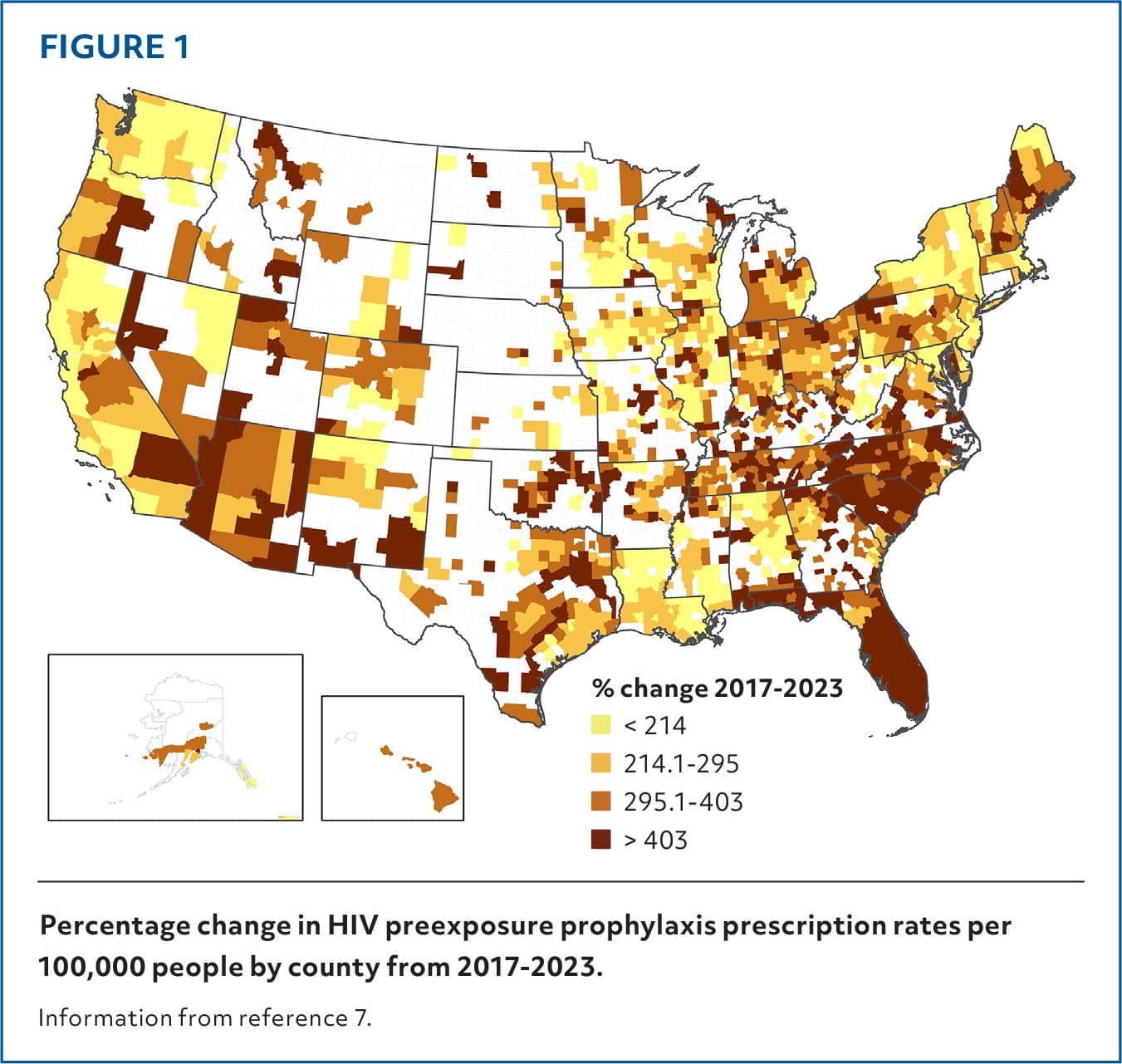
Percentage change in HIV preexposure prophylaxis prescription rates per 100,000 people by county from 2017–2023.
Information from reference 7.
The cost effectiveness of PrEP makes it a wise investment for public health and medical spending.9 This analysis demonstrates that primary care physicians are able and ready to continue providing this essential preventive service. If the US Department of Health and Human Services overturns the USPSTF recommendation, Congress should pass legislation to protect patient access to PrEP without cost sharing.
