
Brain and neurologic health: clinical guidance and practice resources

Cognitive health plays a critical role in patients’ functioning and quality of life across the lifespan, from early neurologic injury to age-related cognitive decline.
Advances in brain health research and evolving diagnostic and management approaches make it essential for family physicians to stay current in caring for patients with cognitive and neurologic concerns.
This page brings together evidence-based clinical guidance and practice resources to support family physicians in the identification, evaluation, and longitudinal management of conditions affecting cognitive health, including dementia, stroke, and traumatic brain injury.
Clinical guidelines and recommendations
Clinical practice guidelines
Action Collaborative on Traumatic Brain Injury Care: Adapted Clinical Practice Guideline
(Endorsed, May 2025)
The Traumatic Brain Injury Action Collaborative Clinical Practice Guideline (CPG) on Management Strategies for Post-Acute Traumatic Brain Injury was developed by the National Academies of Sciences, Engineering, and Medicine (NASEM) and was endorsed by the American Academy of Family Physicians.
Key Recommendations
For patients seeking outpatient care following an incident that involved a plausible mechanism of TBI, qualified health care professionals should attempt to confirm or rule-out a diagnosis of traumatic brain injury based on the 2023 American Congress of Rehabilitation Medicine criteria (ACRM).
Patients should be (re)directed to an ED for urgent evaluation if they have any of the following:
- Declining or fluctuating level of consciousness
- New onset of:
- Pupil asymmetry
- focal neurologic abnormality
- seizures, repeated vomiting
- marked change in behavior
- Severe or worsening headache
- Racoon (panda) eyes, battle’s sign, rhinorrhea/otorrhea or other signs of undiagnosed skull fracture
Health care professionals should not order a brain MRI or CT for every patient but may consider ordering a brain MRI or CT for those with atypical clinical features or symptom course.
Health professionals should screen all patients with TBI for social determinants of health (SDoH), including but not limited to food, housing, and transportation insecurity, transportation needs, financial difficulties, employment-related concerns, migration status, and interpersonal safety.
Health care professionals may provide written and oral information to the patient (and their accompanying family/caregiver) at the initial visit, and ongoing education at subsequent visits.
Health care professionals may screen the following domains for factors that increase the risk of persisting symptoms:
- Demographics
- Pre-existing health conditions
- Indicators of brain injury severity
- High burden post-concussion symptoms on a standardized questionnaire
- Mental health symptoms
- Psychosocial
- Social determinants of health
Health care professionals should prioritize symptoms that are most bothersome to the patient, if treated successfully, are most likely to bring about improvement in other symptoms, and/or impede participation in active rehabilitation.
Health care professionals should characterize the headache history and presentation(s) to determine if the patient has posttraumatic headache with features similar to migraine, tension-type, cervicogenic, and/or other headache types.
Qualified health care professionals should screen for new onset mental health conditions and worsening of pre-existing mental health conditions after TBI.
Referral to specialty care should be considered for patients who are at high risk for persisting symptoms, continue to have disabling symptoms beyond 30 days post-injury, and/or are not responding to first-line interventions in primary care.
Clinical preventive service recommendations
USPSTF concludes there is insufficient evidence to assess whether screening for cognitive impairment in adults aged 65 and older without symptoms results in more benefit than harm. This recommendation applies to community-dwelling older adults who do not exhibit recognized signs of cognitive decline.
USPSTF found insufficient evidence to determine whether screening asymptomatic children aged 5 years or younger for speech and language delays leads to more benefit than harm. This recommendation applies to children without signs, symptoms or parental or clinician concerns about speech, language, hearing or development.
Alzheimer's disease and related dementias (ADRD)
Family physicians occupy a crucial position in brain health. By caring for patients across the life span you are well placed to educate individuals about protecting cognitive function, identify risk factors early and guide patients and families through prevention, early screening, diagnosis and treatment. As the evidence around Alzheimer’s disease and related dementias (ADRD) continues to evolve, you need practical tools that support effective conversations and integrate cognitive care into everyday practice.
The AAFP has developed a collection of brain health resources to support family physicians and their care teams.
Many of these resources also support health literacy by translating complex evidence—such as risk factors linked to cognitive decline—into accessible information that clinicians can use in patient conversations.
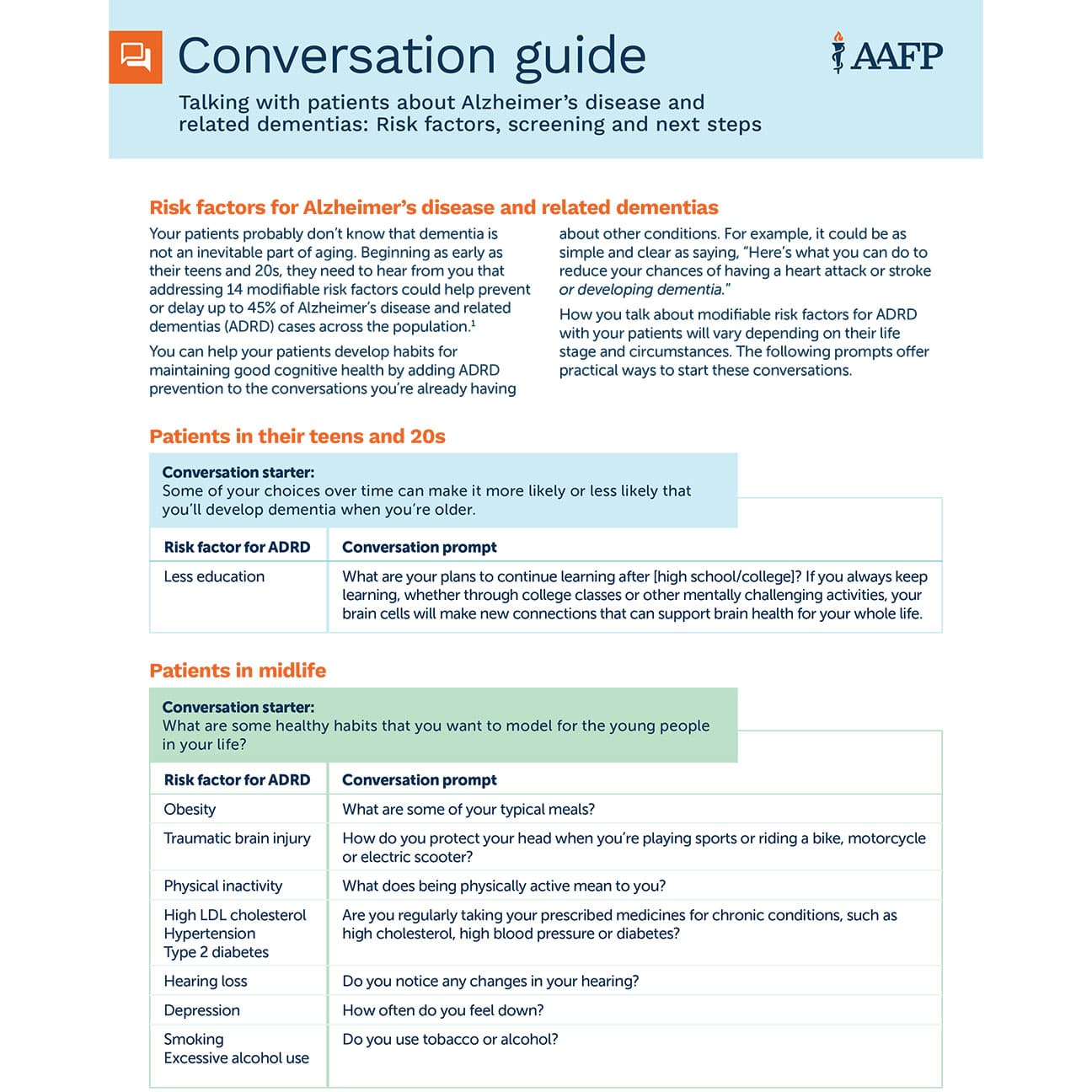
Conversation guides
Chronic conditions
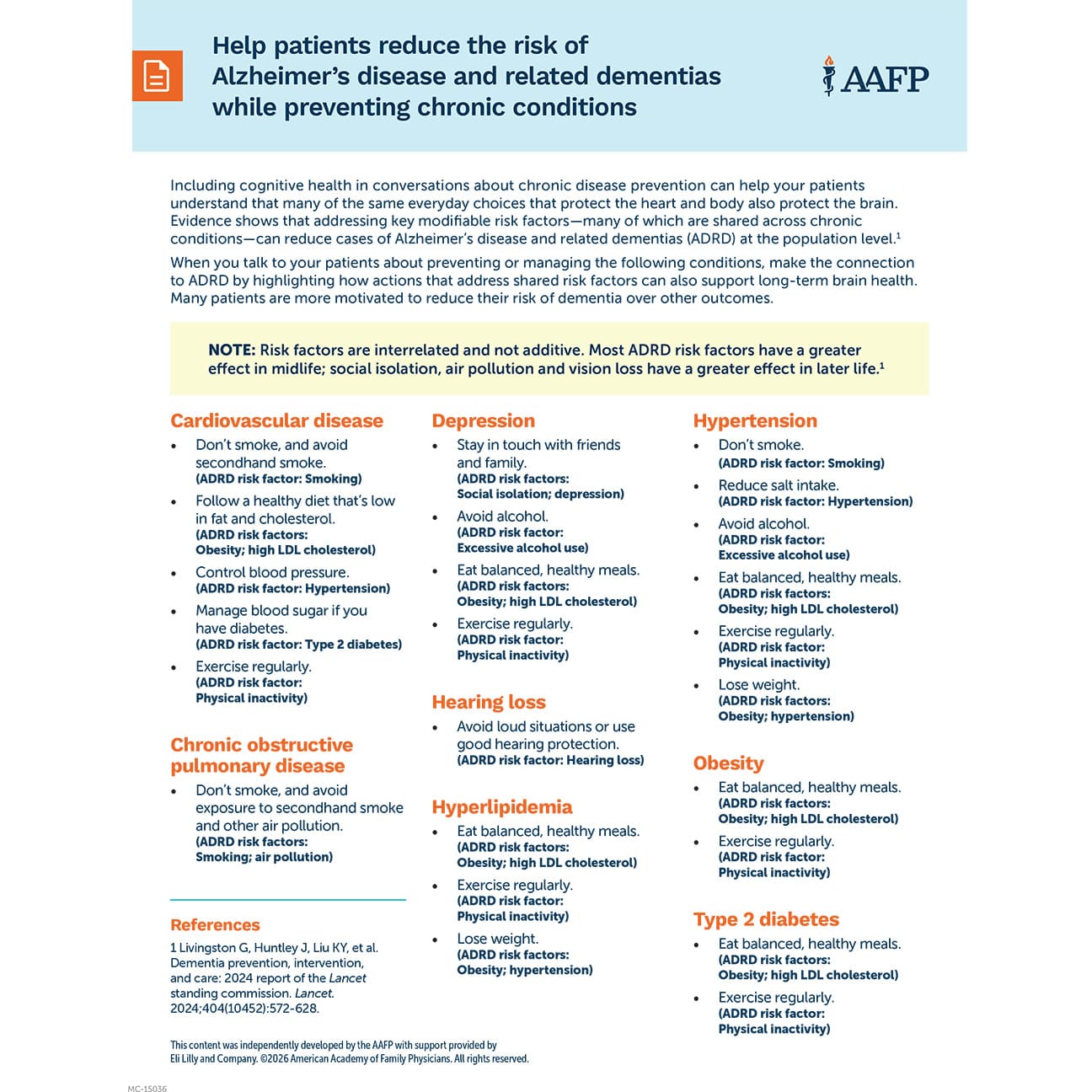
Use this fact sheet to talk to your patients about preventing or managing chronic conditions, making the connection to ADRD by highlighting how actions that address shared risk factors can also support long-term brain health.
Read the full guide.
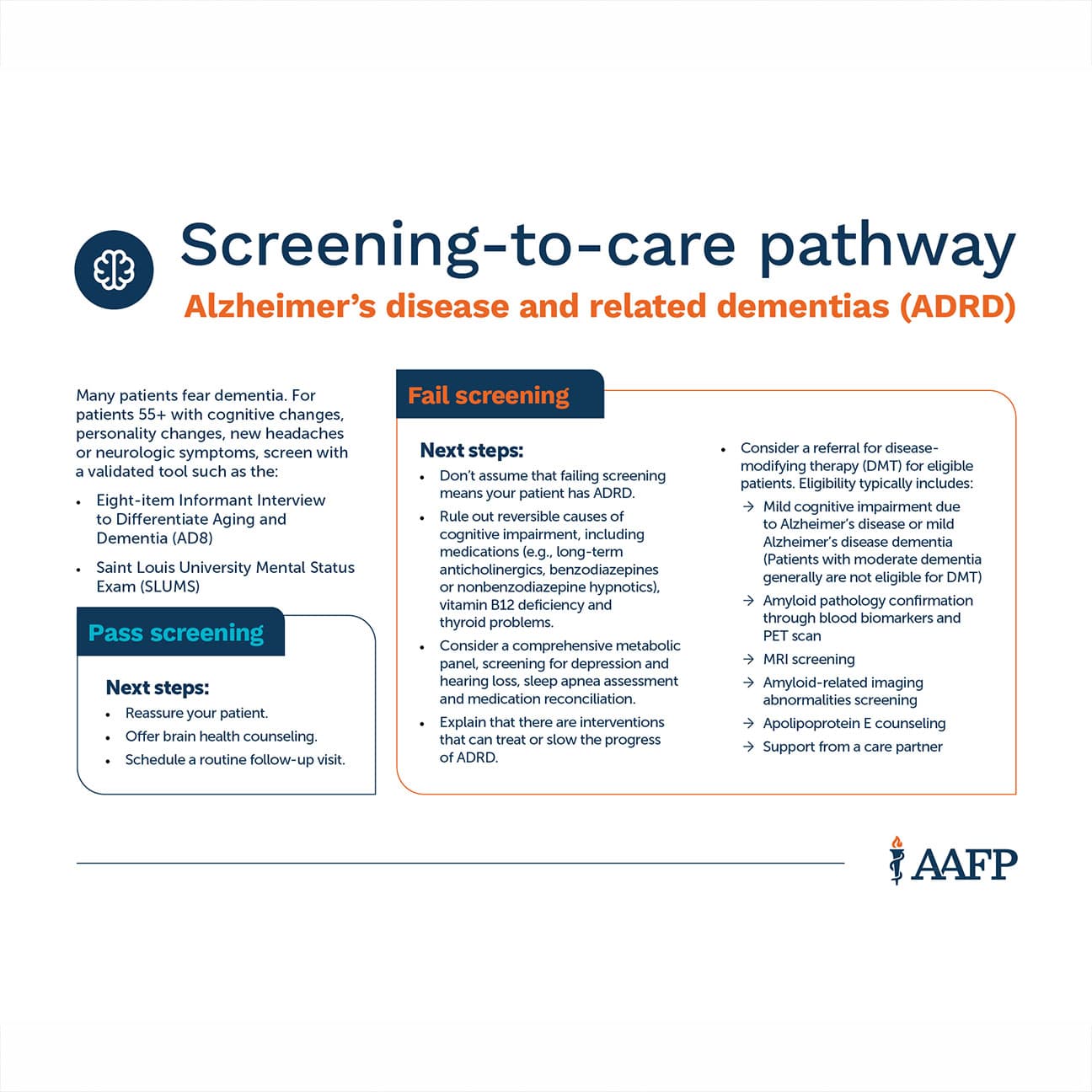
Screening treatment
Read the full guide
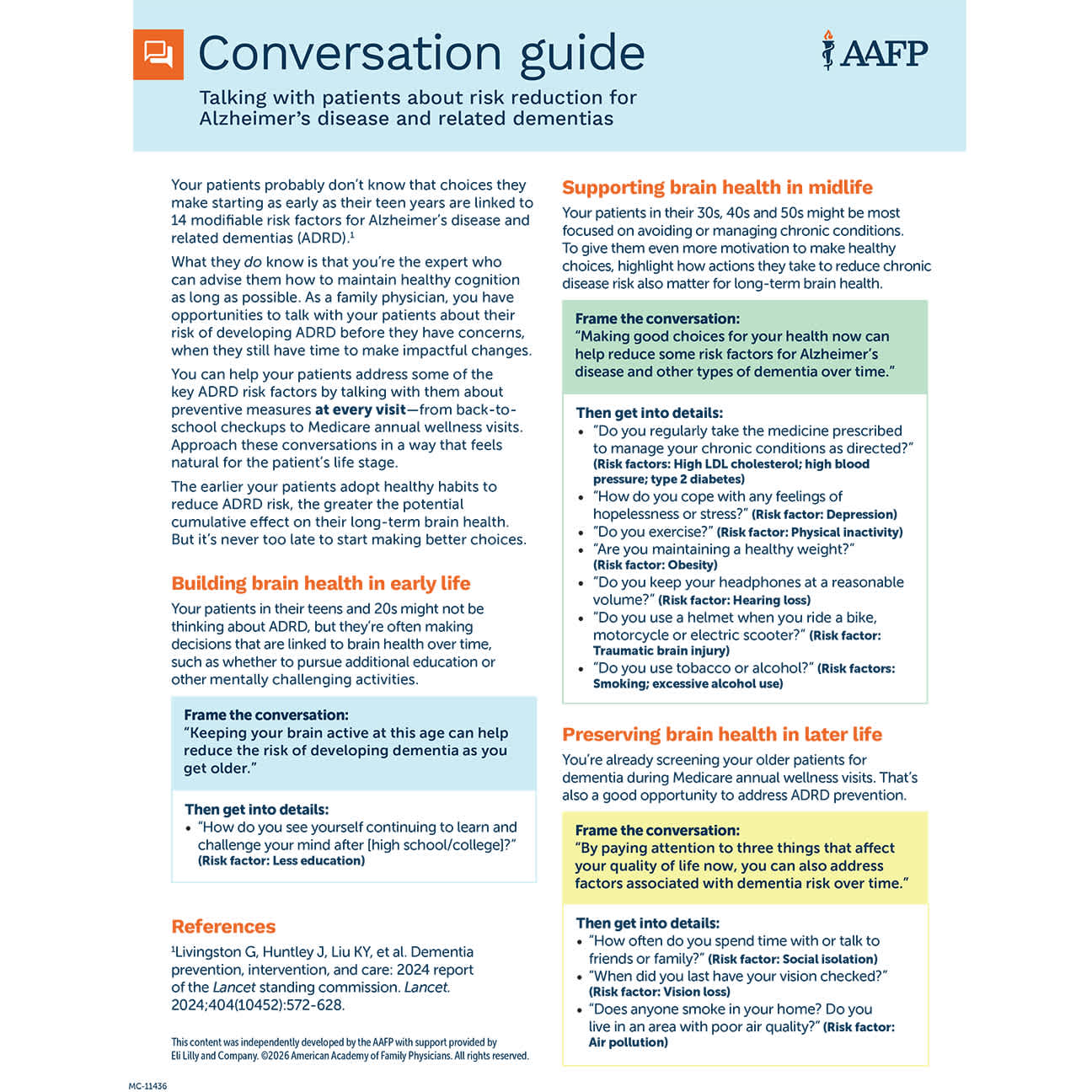
Risk reduction
Read the full guide


Podcasts
Innovative Diagnostic Tools and Workflows for Suspected Alzheimer’s in Primary Care
In this special edition of Inside Family Medicine, sponsored by Roche Diagnostics, host Darren Sextro talks with brain health experts Deanna Willis, MD, MBA, a board-certified family physician, and Jared Brosch, MD, board-certified neurologist, on the use of blood-based biomarkers (BBBMs) in primary care settings for Alzheimer’s disease and related dementias. Their discussion explores how BBBMs can make referrals more efficient and enhance the evaluation of patients with cognitive decline. The conversation highlights the value of early diagnosis and therapy referrals as well as outlines effective workflow strategies for primary care teams.
Primary Care and Cognitive Concerns: Screening, Diagnosis, and Support
Host Michael Monroe interviews Dr. Brianna Wynne, a board-certified geriatric medicine physician, about how family physicians can support prevention, screening, and early detection of cognitive aging and Alzheimer’s disease.
Brain Health and Chronic Conditions: Lifelong Connections
In this episode of ‘Inside Family Medicine’, we hear from Dr. Ariel Cole, a family and geriatric medicine physician and fellowship/residency leader at AdventHealth Orlando, about the family physician’s role in cognitive aging, Alzheimer’s disease and related dementias. Dr. Cole describes her experience caring for patients across the cognitive decline spectrum and emphasizes prevention.