Lumbar spinal stenosis is a clinical syndrome that affects more than 200,000 people in the United States annually. It is a common cause of chronic insidious low back pain, especially in older patient populations (mean age = 64 years). Lumbar spinal stenosis is a degenerative condition of the spine leading to narrowing in the spaces around the neurovascular bundles and the classic symptom of low back pain that radiates to the buttocks and lower extremities bilaterally. It is typically a progressive waxing and waning process that may deteriorate over years. The pain is typically burning or cramping, which worsens with standing and walking and improves with bending forward or sitting. Magnetic resonance imaging is the recommended diagnostic test because it allows cross-sectional measurement of the spinal canal. Options for nonsurgical management include physical therapy, exercise programs, spinal injections with and without corticosteroids, chiropractic treatment, osteopathic manipulation, acupuncture, and lifestyle modifications; however, few of these treatments have high-quality randomized trials demonstrating effectiveness. Surgery may be considered if nonsurgical management is ineffective.
Up to 90% of the U.S. population will experience significant low back pain (i.e., pain requiring the patient to seek medical care or miss work) in their lifetime.1–3 Low back pain becomes chronic in up to 23% of patients and recurs within one year in up to 80%.2,4 Lumbar spinal stenosis is a common cause of chronic low back pain, particularly in people older than 50 years, and is a progressive degenerative condition of the intervertebral disk, ligamentum flavum, and facet joints secondary to aging. It causes a narrowing in the spaces encompassing the neurovascular structures of the spine, leading to the characteristic clinical syndrome of buttock and bilateral lower extremity pain that may include the lower back.3 The pain typically worsens with walking or standing and improves with sitting or leaning forward.5–8 Figure 1 shows normal spinal anatomy.3
SORT: KEY RECOMMENDATIONS FOR PRACTICE
RCT = randomized controlled trial.
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to https://www.aafp.org/afpsort.
FIGURE 1.
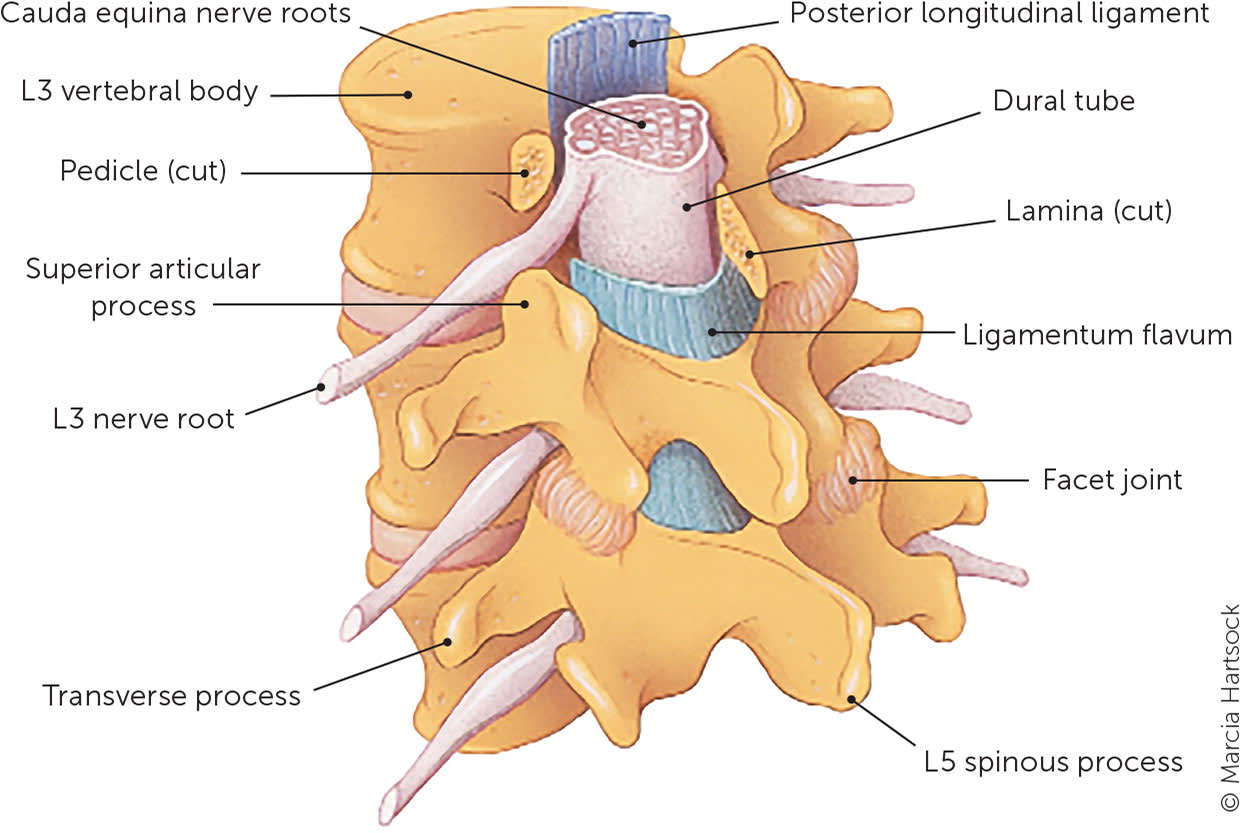
Lower lumbar spine anatomy. The lower lumbar spine carries most of the body weight and is often affected by spinal stenosis. Intervertebral disk degeneration leads to facet loading and degeneration, influencing the attached ligamentum flavum.
Illustration by Marcia Hartsock
Reprinted with permission from Alvarez JA, Hardy RH Jr. Lumbar spine stenosis: a common cause of back and leg pain. Am Fam Physician. 1998;57(8):1826.
A diagnosis of lumbar spinal stenosis is confirmed with radiographic findings of narrowing or stenosis of the lumbar spinal canal or lateral recesses, differentiating it from other similarly presenting causes of low back pain (Table 14,9 ). Because of a lack of evidence to determine the best therapy, initial management includes conservative methods such as oral medications, physical therapy, core strengthening, and injection therapy.6,10,11 Surgical management can be considered if nonsurgical treatment is unsuccessful or the patient has rapidly progressive neurologic symptoms.12–14
TABLE 1. Differential Diagnosis of Lower Extremity Pain With Low Back Pain
| Diagnosis | Symptoms | Physical examination findings* |
|---|---|---|
| Chronic exertional compartment syndrome | Tightness in the calf after exercise usually associated with pain; numbness that progresses to weakness and foot drop | Induced by strenuous exercise and relieved (over time) with limb elevation |
| Hip joint pain | Groin or buttock pain, with or without low back pain; no pain below the knee | Limited internal rotation; positive FADIR test |
| Lumbar nerve root impingement | Radicular pain, with or without low back pain | Positive result on one or more of the following: seated straight leg raise, slump test, supine straight leg raise; decreased peripheral reflexes on the affected side |
| Lumbar spinal stenosis | Low back pain, leg pain, wide-based gait, neurologic weakness | Older age, leg pain more severe than back pain; bilateral symptoms are more typical; pain is worse with standing and walking, relieved with leaning forward or sitting |
| Lumbar vertebral fracture | Low back or thoracic back pain | Tenderness to palpation over the injured vertebra, midline tenderness to palpation; acute onset; usually no history of recent trauma; pain worsened by all activity |
| Muscle strain | Strains or sprains to the hip adductors or abductors (gluteus medius and minimus) and hip flexors, with or without low back pain | Tenderness to palpation over the specific muscle or group; pain and weakness on eccentric testing of the specific muscle group |
| Myofascial referred pain | Pain in the area of involvement | Pain is reproduced with palpation of trigger or pressure points within the target muscles in question, usually the gluteus medius and minimus |
| Peripheral neuropathy | Pain, numbness, and tingling in the distal lower legs and feet that are not affected by posture or exercise | Usually caused by a systemic issue such as diabetes mellitus or thyroid dysfunction |
| Piriformis syndrome | Pain in the buttocks and proximal lower extremity | Pain does not typically radiate below the knee unless the sciatic nerve is being compressed; normal reflexes and strength testing |
| Referred pain from facet joints or intervertebral disks | Pain in the proximal lower extremity | No pain below the knee; normal reflexes and strength testing |
| Sacroiliac joint pain | Low back pain overlying the sacroiliac joint, with or without buttock pain; often worsens with sitting or rising from a seated position | Positive compression test of the sacroiliac joint; tenderness to palpation at the sacroiliac joint and posterosuperior iliac spine; positive distraction test |
| Trochanteric pain syndrome | Lateral hip and thigh pain, with tenderness to palpation over the greater trochanter; low back pain possible | Tightness of the Iliotibial band over the greater trochanter (Ober test) |
| Vascular claudication | Leg pain with cramping, tightness, and fatigue; pain in the buttocks and lower extremity that worsens with activity and is relieved with rest; not affected by posture such as standing or sitting | Decreased pulses in the lower extremities common; impaired ankle-brachial indexes |
| Visceral referred pain | Low back pain, lower extremity pain, or both secondary to pain referred from intra- or extraperitoneal structures (i.e., gastrointestinal and genitourinary structures) | Pain is caused by processes such as uterine fibroids, ovarian cysts, Crohn disease, ulcerative colitis, pyelonephritis, and other gastrointestinal and genitourinary disorders |
FADIR = flexion, adduction, and internal rotation.
*—See Table 4 for test details.
Pathophysiology
Low back pain is pain that extends from the 12th rib to the iliac crest.4 Lumbar spinal stenosis is a common cause of chronic low back pain, particularly in older people, and can be acquired or congenital. The most common is acquired, which results from changes initiated by degeneration of the intervertebral disk during aging. The degeneration and atrophy of the lumbar stabilizing musculature, in combination with repeated daily microtraumas from normal wear and tear, lead to degenerative disk collapse.2,5 This collapse is also thought to be secondary to an imbalance between the catabolic and anabolic processes within the disk, causing extracellular matrix degeneration, neoinnervation, and neovascularization, resulting in disk bulging.15
The collapse of the disk space destabilizes the anterior column, which shifts the axial center of weight to the facet joints, interspinous ligament, and ligamentum flavum. This leads to joint hypertrophy and osteophyte formation, which causes narrowing of the lateral recesses, neuroforamen, or central canal. When this stress becomes significant, it can cause degenerative spondylolisthesis (anterior displacement of a vertebral segment) with or without spondylolysis (defect in the pars interarticularis), which can contribute to lumbar spinal stenosis.9,12 Table 2 lists the causes of central and foraminal lumbar spinal stenosis.2,5,12
TABLE 2. Causes of Central and Foraminal Lumbar Spinal Stenosis
History
Patients with lumbar spinal stenosis can be asymptomatic or present with signs and symptoms ranging from vague low back pain to bilateral leg numbness and weakness. Neurogenic claudication is a cluster of symptoms such as cramping, burning, and tingling that may start in the lower back and move to the buttocks, groin, and anterior thigh and radiate down the posterior part of the legs, causing a perceived loss of balance.1,5,9,13 These symptoms may be unilateral or bilateral and are consistently reproducible with the same activity. Loss of balance associated with low back pain has a 70% sensitivity and 53% specificity for lumbar spinal stenosis.9 Symptoms are typically aggravated by walking or prolonged standing and relieved by bending forward (i.e., shopping cart sign [Figure 2]) or sitting.5,16,17 Patients with low back pain combined with claudicating leg pain that includes bowel and bladder dysfunction, saddle anesthesia, and new or worsening lower extremity weakness should be referred for urgent surgical evaluation.18
FIGURE 2.
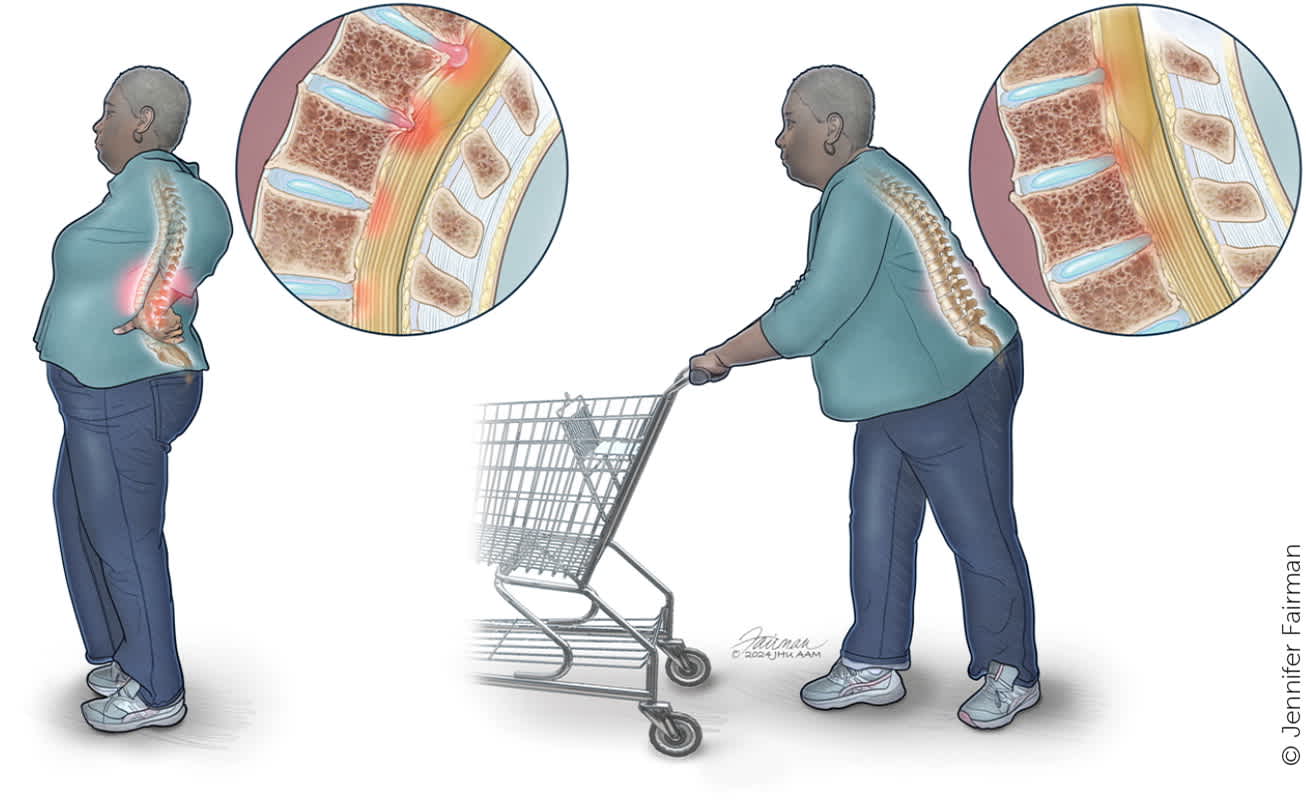
Shopping cart sign. The shopping cart sign, or improvement in pain from lower lumbar stenosis with leaning forward, is due to reduction of disk herniation with reduction in the normal standing lordosis of the lumbar spine.
Illustration by Jennifer Fairman
Physical Examination
The physical examination of patients with suspected lumbar spinal stenosis includes inspection, palpation, range of motion, strength testing, reflexes, and special tests. Inspection assesses for evidence of previous surgeries, spina bifida, and scoliosis, which can cause low back pain. A gait evaluation is necessary because lumbar spinal stenosis typically causes pain with prolonged standing and walking and is characterized by a wide-based gait.4,5,19 A wide-based gait with a positive Romberg sign has a 40% sensitivity and 90% specificity for lumbar spinal stenosis.12
On palpation, the spine is nontender; however, extension usually elicits pain (thigh pain with extension of the spine has a 51% sensitivity and 69% specificity for lumbar spinal stenosis).12 Any decrease in strength, reflexes, or sensation should also be noted (Table 3 and Figure 3). Although there are no specific tests or signs for lumbar spinal stenosis, several tests should be performed to help exclude other diagnoses (Table 41,3,5,13 ). Some of these tests, when combined with other findings, support a diagnosis of lumbar spinal stenosis (i.e., Romberg sign with a wide-based gait). It is important to check distal pulses and the ankle-brachial index to exclude vascular claudication. Table 5 compares the clinical characteristics of vascular and neurogenic claudication.3 The hip joint should be examined because hip pain can mimic low back pain.
TABLE 3. Summary of Nerve Roots
| Nerve root | Reflex | Dermatome* | Myotome | Function |
|---|---|---|---|---|
| L1 | Cremasteric (male); Geigel (female) | Back, groin, pelvis, and inguinal canal | Iliopsoas | Hip flexion |
| L2 | Patellar | Back and front of the thigh starting below the canal to the knee | Iliopsoas | Hip flexion |
| L3 | Patellar | Back, upper buttock, anterior thigh, knee, and medial lower leg | Quadriceps | Knee extension |
| L4 | Patellar | Medial buttock, lateral thigh, medial leg, dorsum of foot, first toe, and medial malleolus | Tibialis anterior | Ankle dorsiflexion |
| L5 | Semimembranosus | Buttock, posterior, lateral thigh, lateral leg, and dorsal foot that includes the sole and the first through fourth toes | Tibialis anterior | Ankle dorsiflexion |
| S1 | Achilles | Buttock, posterior leg or calcaneal area, lateral malleolus, and up the fifth toe | Gastrocnemius and soleus | Ankle plantar flexion |
| S2 | Achilles | Buttock, thigh, posterior leg, and genitals | Gastrocnemius and soleus | Ankle plantar flexion |
*—See Figure 3 for an illustration of lower extremity dermatomes.
FIGURE 3.
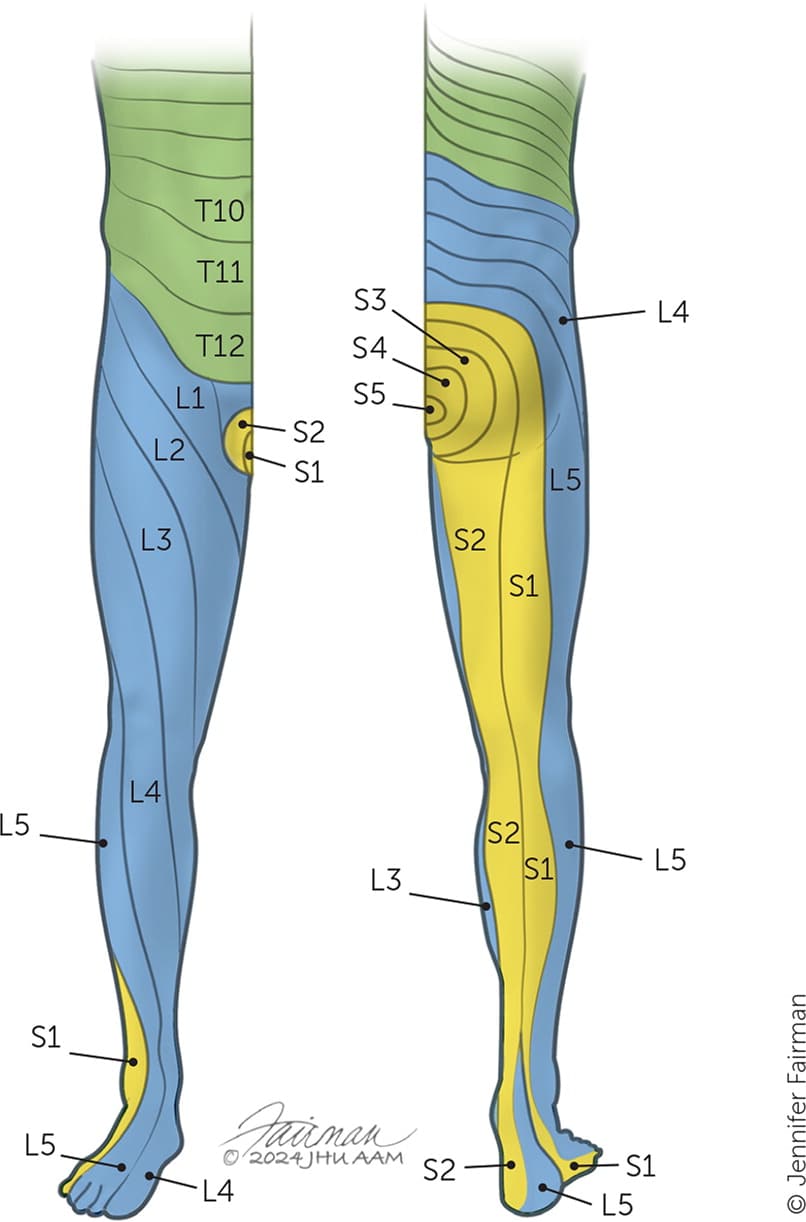
Lower extremity dermatomes.
Illustration by Jennifer Fairman
TABLE 4. Tests to Differentiate Lumbar Spinal Stenosis From Other Diagnoses
| Test | Findings | Diagnosis if positive |
|---|---|---|
| Babinski sign | Using the handle of a reflex hammer, the clinician sweeps up the plantar surface of the patient's foot from the heel up and over to the great toe; upward movement or dorsiflexion of the great toe is positive | Upper motor neuron lesion |
| Buerger test | With the patient supine, the affected leg is lifted between 15 and 30 degrees for 30 to 60 seconds; if pallor occurs, the test is positive for vascular insufficiency | Peripheral vascular disease |
| Compression test of the sacroiliac joint | With the patient in the lateral recumbent position, the clinician places a hand on the anterosuperior iliac spine and iliac crest of the patient's upward side, then presses toward the floor; a positive test elicits pain at the sacroiliac joint | Sacroiliac joint dysfunction |
| Crossed straight leg raise test | The clinician raises the contralateral leg (opposite leg to the sciatic symptoms) to 60 degrees of hip flexion while the patient is supine; reproduction of the radicular symptoms down the contralateral leg below the knee is considered a positive result and has a 35% sensitivity and 90% specificity for nerve root impingement | Nerve root impingement at the spine |
| Distraction test (squish test) | With the patient in the supine position, the clinician places their hands on the anterosuperior iliac spine and produces a downward force toward the sacroiliac joint; a positive test elicits pain at the sacroiliac joint | Sacroiliac joint dysfunction |
| Flexion, adduction, and internal rotation test (anterior apprehension test) | With the patient in the supine position, the clinician takes the affected hip into full flexion, external rotation, and full abduction to start, then as the hip extends, they also take the hip into full internal rotation and adduction; a positive result is indicated by groin pain | Hip impingement syndrome, iliopsoas tendonitis, or anterior labral tear |
| Hoffmann sign | Flicking of the middle fingernail while the patient is seated elicits flexion of the thumb and index finger | Upper motor neuron lesion, usually in the cervical spine |
| Kemp test | The patient extends the back and rotates at the same time; a positive test elicits pain, numbness, and tingling in the concerned area | Lumbar spine facet arthropathy |
| Patrick sign | Reproduced leg pain with lateral rotation of the flexed knee indicates degenerative hip joint disease | Arthritis of the hip joint |
| Piriformis test | With the patient in the lateral recombinant position and the involved side up, the involved hip is flexed to 60 degrees with the knee flexed; the clinician stabilizes the hip with one hand and pushes the knee down with the other hand; a positive test elicits pain in the piriformis muscle and potentially down the thigh if sciatica is present | Piriformis syndrome |
| Seated straight leg raise | With the patient seated and the knees and hips at 90 degrees, the clinician passively extends the knee; if pain is elicited below the knee, the test is positive | Nerve root impingement of the lumbar spine, usually from a herniated disk |
| Slump test | The patient is seated on the table and asked to slump, chin to the chest, then the knee is placed passively in extension and the ankle is dorsiflexed; if pain radiates below the knee, the test is positive | Nerve root impingement of the lumbar spine |
| Supine straight leg raise (Lasègue sign) | The leg is elevated to at least 30 to 40 degrees while the patient is supine; performing this straight leg test while dorsiflexing the foot at the same time may elicit ipsilateral radicular pain radiating distal to the knee, suggesting nerve root compression | Nerve root impingement in the lumbar spine, usually from a herniated disk in a narrowed foramen |
| Tightness of the iliotibial band over the greater trochanter (Ober sign) | With the patient in the lateral recombinant position and the involved leg up, the clinician passively abducts and extends the involved leg with the knee flexed at 90 degrees, then lowers the leg; if the knee does not fall to the level of the opposite knee, then the iliotibial band is tight, and the test is positive | Iliotibial band syndrome |
| Trendelenburg test | Weakness in the gluteal abductors affecting L5 to S2; can be affected by lumbar spinal stenosis | Nerve impairment of the L5 to S2 nerve roots |
TABLE 5. Clinical Differentiation Between Neurogenic and Vascular Claudication
| Clinical characteristics | Neurogenic claudication | Vascular claudication |
|---|---|---|
| Location of pain | Thighs, calves, back, and rarely buttocks | Buttocks or calves |
| Quality of pain | Burning, cramping | Cramping |
| Aggravating factors | Erect posture, ambulation, extension of the spine | Any leg exercise |
| Relieving factors | Squatting, bending forward, sitting | Rest |
| Autonomic changes | Bladder incontinence (rare) | Impotence may coexist with other symptoms of vascular claudication |
| Leg pulses and blood pressure | Usually normal | Blood pressure decreased; pulses decreased or absent; bruits or murmurs may be present |
| Skin/trophic changes | Usually absent | Pallor, cyanosis, and nail dystrophy often present |
Adapted with permission from Alvarez JA, Hardy RH Jr. Lumbar spine stenosis: a common cause of back and leg pain. Am Fam Physician. 1998;57(8):1825–1834.
Imaging
Most patients presenting with lumbar spinal stenosis are older than 50 years; therefore, plain radiography of the lumbar spine typically reveals degenerative changes (Figure 4). Magnetic resonance imaging (MRI) provides the most diagnostic information for patients with lumbar spinal stenosis symptoms because it allows for cross-sectional measurement of the spinal canal2,5,20,21 (Figure 5). However, for lumbar spinal stenosis to be diagnosed, the patient must have clinical symptoms and radiologic confirmation of spinal stenosis (central or foraminal).5,12,13,16
FIGURE 4.
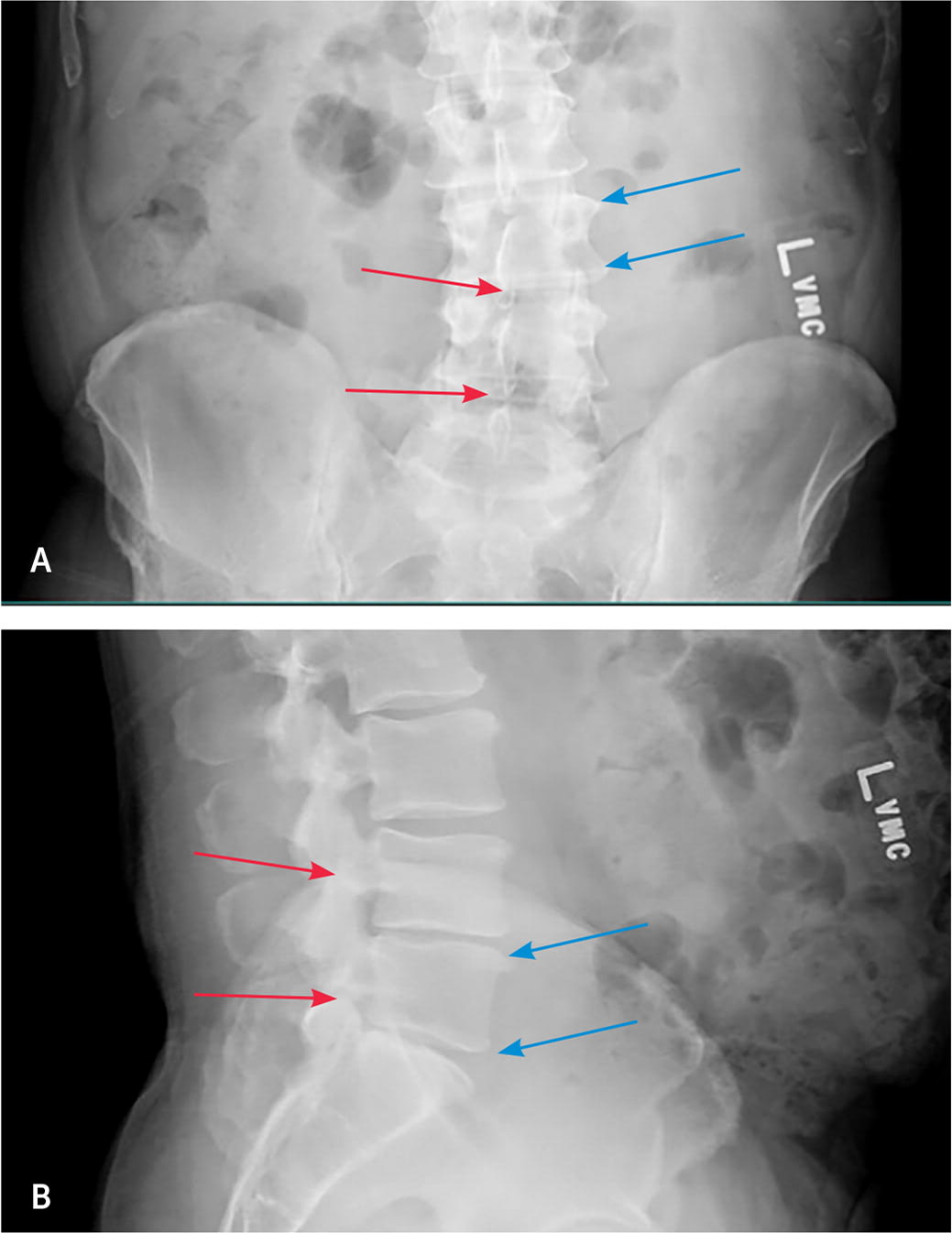
Radiographs in a patient with L5 to S1 right-sided disk herniation. (A) Anteroposterior view. Note the vertebral endplate irregularities (blue arrows), the minimal scoliotic curve, and the loss of disk height in L4 to L5 and L5 to S1 (red arrows). (B) Lateral view. Note the multilevel degenerative disk disease demonstrated by endplate abnormalities and the loss of disk height worse at L4 to L5 and L5 to S1 (blue arrows), the mild to moderate facet arthropathy (red arrows), and the reduction in the normal lordotic curve.
FIGURE 5.
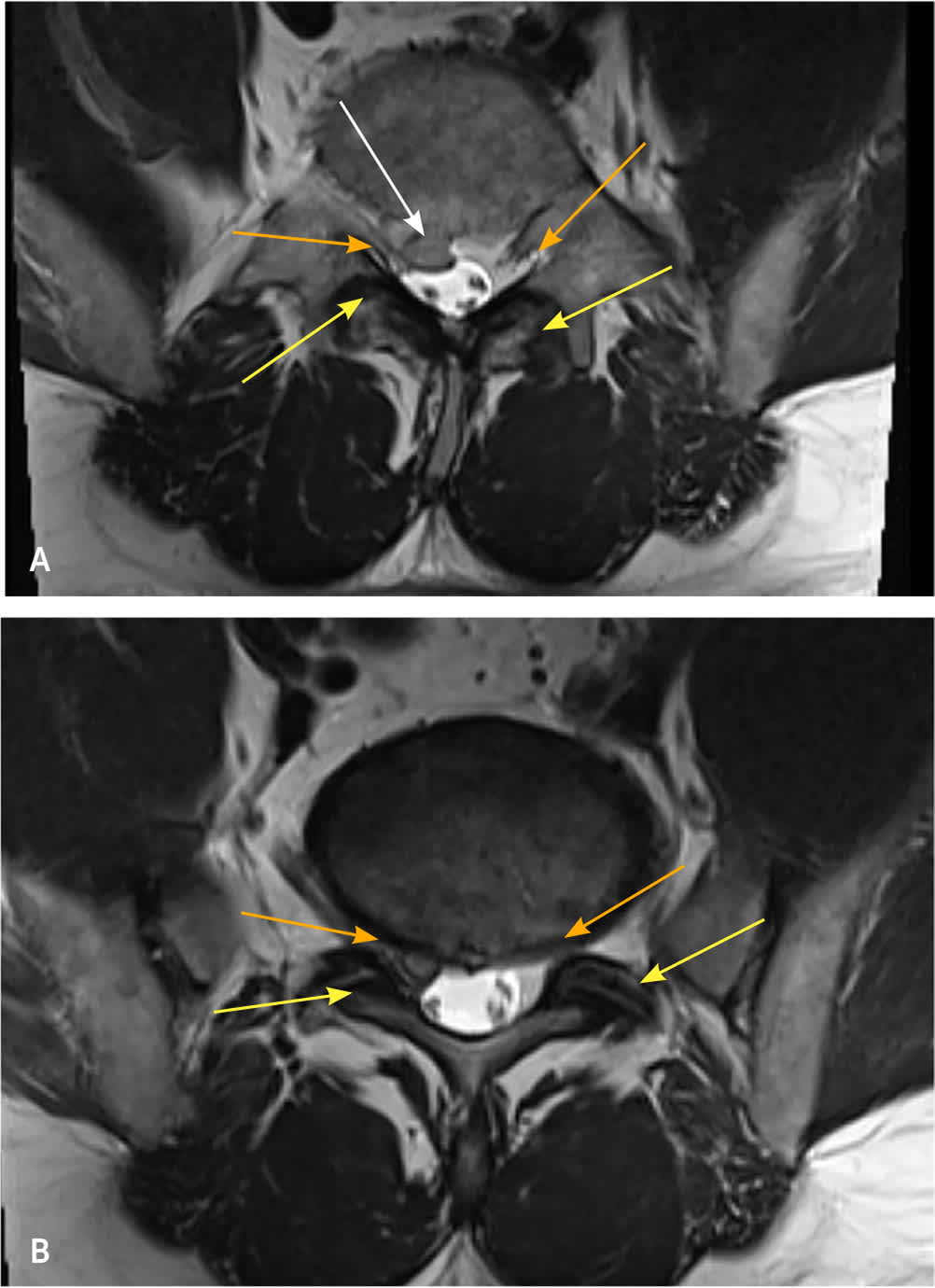
Magnetic resonance imaging scan showing axial view of the lumbar spine. (A) Central canal stenosis with nerve root impingement by herniated intravertebral disk (white arrow), facet hypertrophy (yellow arrows), and foraminal narrowing (orange arrows). (B) Bilateral facet hypertrophy (yellow arrows) with narrowing of the lateral recesses causing nerve root impingement (orange arrows).
Computed tomography myelography is recommended if MRI cannot be performed (e.g., the patient has spinal or cardiac instrumentation or other hardware that may not be MRI compliant).9 Other testing includes electromyography and nerve conduction studies. However, these are not used routinely and are usually reserved for differentiating lumbar spinal stenosis from osteoarthritis, vascular claudication, and other spinal cord lesions.5,22
Treatment
Evidence-based recommendations for the treatment of lumbar spinal stenosis are complicated by heterogeneity of the condition, a waxing and waning nature, and lack of high-quality studies evaluating its treatment exclusively (many of the studies of lumbar spinal stenosis overlap with other etiologies of chronic low back pain).23 The general options are nonoperative treatment vs. surgery. Few high-quality randomized trials have investigated differentiated approaches to nonoperative treatment, which include medications, physical therapy, bracing, alternative/complementary medicine, and epidural injections. Studies comparing operative vs. non-operative therapy often poorly describe the treatment of the nonoperative group.10 Even in trials where investigators successfully categorized the nonoperative treatment arm, the significant crossover between the operative and nonoperative groups hampers interpretation of the results.11
PHARMACOLOGIC
Medications historically used to treat lumbar spinal stenosis include acetaminophen, nonsteroidal anti-inflammatory drugs (NSAIDs), muscle relaxants, opioids, neuromodulators, corticosteroids, antidepressants, and calcitonin. A Cochrane review of two randomized controlled trials (RCTs) found that acetaminophen was not superior to placebo for reducing pain and disability in the short or long term. However, this study was not limited to lumbar spinal stenosis and included low back pain of differing etiologies.24 A meta-analysis of six trials comparing NSAIDs with placebo had similar limitations but found significant short-term pain relief with NSAIDs in patients with chronic low back pain.25 A more recent Cochrane review of the pharmacologic treatment of low back pain (also not specific to lumbar spinal stenosis) found that NSAIDs, muscle relaxants, and opioids had a small effect on pain reduction, but use of muscle relaxants and opioids was complicated by a significant risk of adverse effects.26 A systematic review found no clinically significant difference in pain control between NSAIDs and opioids.27
A small RCT found that adding gabapentin to physical therapy, bracing, and NSAIDs improved pain control in patients with lumbar spinal stenosis.28 Significant adverse effects in 40% of treated patients may limit the use of gabapentin.29 The antidepressant duloxetine (Cymbalta) has been shown to improve chronic low back pain compared with placebo, but the studies did not include lumbar spinal stenosis.30,31 In patients with lumbar spinal stenosis, nasal calcitonin has not been shown to significantly improve pain or function.32 Patients must weigh the risks of adverse effects with the potential benefits of pain relief when considering any medication for the treatment of lumbar spinal stenosis.
Two RCTs demonstrated that epidural corticosteroid injections with lidocaine improve pain and function after 3 weeks compared with lidocaine alone. Epidural corticosteroid injections should only be considered for short-term pain relief, and clinicians should consider epidural lidocaine injections without the addition of corticosteroids.33,34
NONPHARMACOLOGIC
Exercise and physical therapy are options to decrease pain and improve walking distance in the short term, but there is no robust evidence for these treatments.8 Bracing with a lumbosacral orthosis may decrease pain and increase walking distance.35 There is conflicting evidence from low-quality trials on the effects of acupuncture on lumbar spinal stenosis.36,37 Larger studies are needed to determine whether acupuncture has promise as treatment. More studies are also needed to evaluate the use of transcutaneous electrical nerve stimulation and manipulation (chiropractic and osteopathic) to treat lumbar spinal stenosis.35
SURGICAL INTERVENTIONS
Surgical options for the treatment of lumbar spinal stenosis include decompression, decompression with fusion, percutaneous implantation of an interspinous spacer device, and minimally invasive lumbar decompression. Surgery is more effective than nonoperative therapy in improving short- and long-term pain, especially if leg symptoms are predominant; however, surgery is also associated with a higher risk of complications.6,38–40 A trial demonstrated greater improvement in pain, function, and self-reported progress at 8 years with surgery compared with nonoperative treatment. However, the convergence of outcomes between the treatment groups after 5 years was significant, and a large loss of patients to follow-up is suspected to have biased the treatment effect calculations.41 In a more recent meta-analysis, there were no differences between operative and nonoperative approaches in short-term functional outcomes at 6 months, and there were increased complications in patients treated surgically. At 1 year, functional outcomes appear to be improved with postsurgical intervention.6,38–40
Studies evaluating decompression techniques could not conclude whether one technique was superior.42 In patients without spondylolisthesis or lumbar scoliosis, fusion with decompression does not improve outcomes over decompression alone.35,43 Meta-analyses evaluating percutaneously placed interspinous spacer devices found that although there may be some benefit in patients without spondylolisthesis who have extension-based neurogenic claudication, there are high rates of complications and reoperation.44,45 Case series and cohort studies have evaluated minimally invasive lumbar decompression, which appears to be successful in decreasing the patient's length of hospitalization, blood loss, and tissue damage; however, these findings must be balanced against the higher complication rates.46,47 More research is needed to determine the effectiveness, safety, and cost-effectiveness of interspinous spacer devices and minimally invasive lumbar decompression.
Clinicians should discuss a range of nonoperative treatment options with their patients and consider surgical referrals for patients whose symptoms are refractory or worsen over time.
This article updates previous articles on this topic by Snyder, et al.,48 and Alvarez and Hardy.3
Data Sources: A PubMed search was completed in Clinical Queries using the key terms lumbar spinal stenosis and spinal stenosis. The search included meta-analyses, randomized controlled trials, clinical trials, and systematic reviews. The Agency for Healthcare Research and Quality, the Cochrane database, and Dynamed were also searched. The Essential Evidence Plus summary was also used as a reference source. This list was cross-referenced with the search results to ensure the articles were part of the essential evidence collection. Whenever possible, studies that did not define how race or gender categories were assigned were not used in our final review. Search dates: April 6 and 13, 2023, and February 6, 2024.
