Chronic low back pain, defined as lumbar pain persisting for 12 weeks or more, occurs in about 13% of U.S. adults. Patients with chronic low back pain should have a history and physical examination to identify red flags that may indicate serious conditions that warrant immediate intervention or yellow flags (i.e., psychological, environmental, and social factors) that indicate risk of disability. The examination should include an evaluation for radicular symptoms. Routine imaging is not recommended but is indicated when red flags are present, there is a neuromuscular deficit, or if pain does not resolve with conservative therapy. Patients should avoid bed rest. Nonpharmacologic treatment is first-line management and may include therapies with varying evidence of support, such as counseling, exercise therapy, spinal manipulation, massage, heat, dry needling, acupuncture, transcutaneous electrical nerve stimulation, and physical therapy. Pharmacologic interventions are second-line treatment. Nonsteroidal anti-inflammatory drugs are the initial medication of choice; duloxetine may also be beneficial. Evidence is inconclusive to recommend the use of benzodiazepines, muscle relaxants, antidepressants, corticosteroids, insomnia agents, anticonvulsants, cannabis, acetaminophen, or long-term opioids. Epidural corticosteroid injections are not recommended except for short-term symptom relief in patients with radicular pain. Most patients with chronic low back pain will not require surgery; evaluation for surgery may be considered in those with persistent functional disabilities and pain from progressive spinal stenosis, worsening spondylolisthesis, or herniated disk. Physicians should consider prevention of chronic low back pain when patients present with acute back pain. Screening tools are available to predict the progression from acute to chronic low back pain, and targeted treatment strategies are beneficial for preventing progression.
Low back pain is a common reason for adults to visit their physician. Based on a systematic review of 165 studies from 54 countries, the lifetime prevalence of low back pain is approximately 40%.1 Globally, low back pain is the most prevalent and disabling condition that benefits from rehabilitation and is the highest generator of health care expenditure and disability.2–4
SORT: KEY RECOMMENDATIONS FOR PRACTICE

NSAIDs = nonsteroidal anti-inflammatory drugs.
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to https://www.aafp.org/afpsort.
Approximately 70% to 90% of lower back pain is self-limited and will improve in six weeks to six months regardless of treatment.5,6 Patients who are consistently symptomatic at four weeks are more likely to develop chronic low back pain.5 In the United States, 13% of adults have chronic low back pain, and 30% of those patients experience significant disability and pain that affects quality of life.7
Chronic low back pain is defined as persistent lumbar pain for 12 weeks or more, with or without sciatica.8 It can be classified as mechanical, radicular (neuropathic), or idiopathic/nonspecific. The most common cause of chronic low back pain is idiopathic/nonspecific, accounting for 70% of cases.9 Because there is a wide range of causes, physicians should be aware of new, acute conditions that can exacerbate ongoing chronic low back pain.10 Table 1 shows the differential diagnosis, red flags, and evaluation of chronic low back pain.9,11–21
TABLE 1. Differential Diagnosis, Red Flags, and Evaluation of Chronic Low Back Pain
| Condition | Risk factors | Symptoms11 | Red flags12–14 | Physical examination findings | Suggested evaluation |
|---|---|---|---|---|---|
| Mechanical | |||||
| Lumbar strain or sprain | Abrupt movement Strenuous activity |
Axial low back pain Occasional referral of pain |
— | Muscle guarding No focal neurologic findings Paraspinal muscle spasm Reduced range of motion |
Not routinely needed |
| Chronic fracture | History of osteoporosis Older age Younger patients at risk of stress fracture (overuse) |
Low back pain with or without upper leg pain | Chronic use of corticosteroids Older age Recent fall |
Midline tenderness No focal neurologic findings |
Lumbosacral plain radiography For inconclusive results, advanced imaging may be indicated |
| Facet joint | Osteoarthritis Spondylolisthesis |
Axial low back pain Referred pain to hip or upper leg is common |
— | Paraspinal tenderness Reduced range of motion No focal neurologic findings |
Not routinely needed |
| Disk disruption | Older age Repetitive injury |
Low back pain or leg pain Pain worse with sitting |
— | Midline tenderness Reduced range of motion No focal neurologic findings |
Not routinely needed |
| Spondylolysis15 | Adolescent age Younger athletes |
Low back pain exacerbated by repetitive motion usually related to sporting activities | — | Limited lumbar range of motion Pain with hyperextension |
Lumbosacral plain radiography Plain CT |
| Neoplasia | Age > 50 years History of cancer Multiple risk factors present |
Unexplained weight loss | History of cancer Unexplained weight loss |
Midline tenderness | MRI* Lumbosacral plain radiography CBC, ESR, and CRP levels |
| Radicular | |||||
| Spinal stenosis16 | Congenital Degenerative spondylolisthesis Disk bulging Facet joint hypertrophy Older age |
Back pain with radicular symptoms or sciatica Lower extremity paresthesia Pain exacerbated by lumbar extension |
Neurogenic claudication (i.e., intermittent lower extremity pain due to nerve impingement)17 | Neurologic findings depending on nerve root involvement Pain relief with bending or sitting Wide-based gait |
Not routinely needed MRI if neurologic deficits are severe or progressing* |
| Herniated disk | Frequency peaks at 30 to 50 years of age Heavy lifting Trauma |
Back pain with radicular symptoms or sciatica Lower extremity paresthesia |
— | Dermatomal pain location Crossed straight-leg raising test Ipsilateral straight leg–raising test Neurologic findings depending on nerve root involvement |
Not routinely needed MRI if neurologic deficits are severe or progressing* |
| Cauda equina syndrome or conus medullaris syndrome18–20 | Intraspinal lesion (variety of causes) | Low back pain with pain radiating down one or both legs Neurologic deficits present as weakness of plantar flexion (S1 and S2) and bladder and rectal sphincter involvement (S3 though S5) Sensory deficit over buttocks, perineum, and upper posterior thigh |
Acute onset urinary retention Loss of anal tone Saddle anesthesia Severe or progressive lower extremity neurologic deficits Urinary or fecal incontinence |
Decreased lower extremity strength and reflexes Decreased rectal tone and anal sphincter contraction |
Emergent MRI† |
| Idiopathic/nonspecific | |||||
| Infection | Immunosuppression | Back pain with fever | Fever or intravenous drug use | Midline tenderness | MRI* CBC, ESR, and CRP levels |
| Inflammatory low back pain | Human leukocyte antigen B27 [corrected] | Alternating buttock pain Improvement with exercise Morning stiffness Younger age |
Awakening due to low back pain | Restriction of spinal mobility in advanced disease | Radiography of pelvis, sacroiliac joint, and spine area of interest |
Note: Overlap exists between mechanical, radicular, and idiopathic/nonspecific causes, and co-occurrence is common.
CBC = complete blood count; CRP = C-reactive protein; CT = computed tomography; ESR = erythrocyte sedimentation rate; MRI = magnetic resonance imaging.
*—MRI should be performed, with or without contrast media, unless it is contraindicated (e.g., renal insufficiency).
†—MRI should be performed unless it is contraindicated (e.g., patients with pacemakers), otherwise, perform CT or CT myelography.
An algorithm outlining the general approach to the treatment of chronic low back pain is shown in Figure 1.5,7,22–26 Key management recommendations from professional organizations are listed in Table 2.
FIGURE 1.
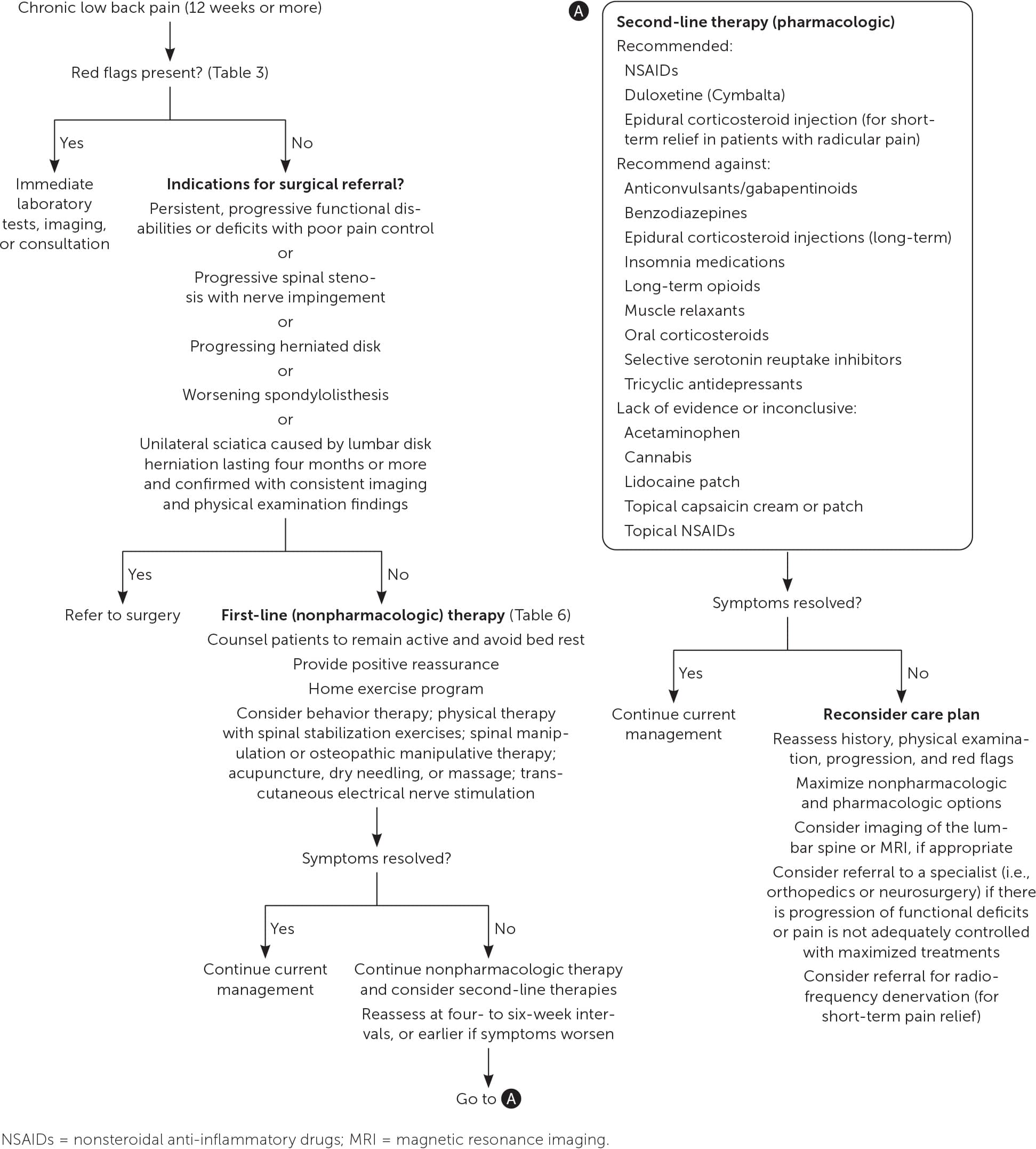
Suggested approach to the treatment of chronic low back pain.
TABLE 2. Professional Organization Recommendations for Managing Chronic Low Back Pain
| Organization | Recommendation |
|---|---|
| American Academy of Family Physicians | Do not perform imaging for low back pain in the first six weeks unless red flags are present. |
| American Academy of Orthopedic Surgeons | Avoid routine use of opioids for lower back pain. |
| American College of Physicians | Do not obtain imaging studies in patients with nonspecific low back pain. |
| North American Spine Society | Do not use electromyography and nerve conduction studies to determine the cause of axial lumbar, thoracic, or cervical spine pain. Do not recommend bed rest for low back pain; patients should remain as active as possible and be encouraged to find positions of comfort and engage in activities that do not worsen symptoms during an acute episode. Do not prescribe opioids for acute or chronic low back pain before a comprehensive evaluation, consideration of a trial of alternative medications and treatments, and discussion of the risks of opioid therapy. |
Source: For supporting citations and to search Choosing Wisely recommendations relevant to primary care, see https://www.aafp.org/afp/recommendations/search.htm.
Evaluation
The clinical evaluation of a patient with chronic low back pain should include a history and physical examination to identify potential red flags that may require immediate intervention. Psychological, environmental, and social risk factors for disability are referred to as yellow flags.27 Table 3 outlines red and yellow flags associated with chronic low back pain.11,27 Patients with more intense pain, obesity, depression, poor coping skills, or anxiety, and those who smoke or perform high-intensity physical labor are at a higher risk of developing chronic low back pain. Regular physical exercise is a protective factor.28
TABLE 3. Red and Yellow Flags Associated With Chronic Low Back Pain
| Red flags (TUNA FISH mnemonic) Trauma Unexplained weight loss Neurologic findings Age > 50 years Fever Intravenous drug use Steroid use History of cancer | Yellow flags Belief that pain and activity are harmful Compensation claims and prolonged sick leave Depressed mood and social withdrawal Exaggerated illness response Lack of support Overprotective family |
PHYSICAL EXAMINATION
The physical examination should include a focused neuro-muscular examination, including reflexes, muscle strength, and sensation. Strength should be evaluated with active knee extension (which is dependent on nerve root L4), and walking on the heels (nerve root L5) and toes (nerve root S1) should be observed.11
Radicular symptoms should be evaluated using the maneuvers listed in Table 4.5 Testing should include the ipsilateral straight leg–raising test and crossed straight-leg raising test. For disk herniation that involves the L5-S1 nerve root, the ipsilateral straight leg–raising test is 92% sensitive and 28% specific, and the crossed straight-leg raising test is 28% sensitive and 90% specific.29–31
TABLE 4. Physical Examination Maneuvers and Findings That Suggest Radiculopathy
| Straight leg raise test: Passive lifting of the affected leg by the examiner to an angle less than 60 degrees reproduces pain radiating distally to the knee |
| Crossed straight leg raise test: Passive lifting of the unaffected leg reproduces pain in the affected (opposite) leg |
| Diminished or absent patellar (L4 or L5 nerve root) or Achilles (S1 nerve root) reflex |
| Weakness of knee extension and ankle dorsiflexion (L4 nerve root), hallux extension and ankle plantar flexion (L5 nerve root), or ankle plantar flexion (S1 nerve root) |
| Sensory deficits in medial leg or foot (L4 nerve root), lateral leg or foot (L5 nerve root), or lateral side of foot (S1 nerve root) |
Reprinted with permission from Chou R. Low back pain. Ann Intern Med. 2021;174(8):ITC117.
LABORATORY TESTS
Laboratory assessment is not routinely needed in chronic low back pain. If a serious condition is suspected, such as cancer, infection, or an inflammatory disorder, physicians should consider obtaining a complete blood count, erythrocyte sedimentation rate, C-reactive protein levels, comprehensive metabolic panel, or other laboratory tests as clinically indicated.5,32
IMAGING
Routine imaging is not recommended in chronic low back pain without clinical indications because systematic reviews have demonstrated inconsistent findings between abnormal imaging and symptomatology.33–35 Imaging should be obtained when chronic low back pain, with or without nerve root involvement, does not resolve with conservative therapy, red flags are present, or there is neuromuscular deficit.36
Physicians should be cautious about the language they use when sharing imaging results with patients because technical or catastrophizing language may result in patients experiencing more pain, less self-efficacy, and poorer function. Patients who are informed that their results are normal, with age-related findings, tend to respond better to treatment and have less pain, improved self-efficacy, and higher function.37
ELECTROMYOGRAPHY
Electromyography can be considered in patients with chronic lower extremity symptoms to evaluate for myelopathy, radiculopathy, neuropathy, and myopathy.5 However, the use of electromyography in the absence of any detectable neuromuscular deficit (e.g., radicular pain, muscle weakness, sensory loss, muscle atrophy) has low-yield value and usually has normal results.38
Nonpharmacologic Treatment
In the absence of conditions that require specific medical or surgical attention, nonpharmacologic treatments are the first-line choice for management of chronic low back pain22,36 (Table 522,39–45 ). The goal of these treatments is to relieve pain and improve function and quality of life.
TABLE 5. Nonpharmacologic Treatment of Chronic Low Back Pain
| Intervention | Contraindications | Frequency |
|---|---|---|
| Educational22,39 (e.g., cognitive behavior therapy, mindfulness-based stress reduction) | — | Two to four times per month for six months |
| Exercise40 (e.g., aerobic, aquatic, Pilates, strength training, structured walking program, tai chi) | Acute congestive heart failure Recent myocardial infarction or complete heart block Unstable angina Uncontrolled hypertension | Once per day |
| Manual therapies41,42 (e.g., osteopathic manipulative therapies, including high-velocity low-amplitude techniques for spinal manipulation) | Acute whiplash Cauda equina syndrome Fractures Fused spinal joints Herniated disk Joint instability Metastasis to the bone Osteoporosis Osteomyelitis Postsurgical Pregnancy Severe rheumatoid arthritis Vertebral artery ischemia | One or two times per month or as needed |
| Lumbar supports43 | Cardiopulmonary restrictions Pregnancy Rash in the covered area | Once per day or until pain improves |
| Electrical nerve stimulation44 (e.g., percutaneous nerve stimulation, transcutaneous electrical nerve stimulation) | Deep venous thrombosis Epilepsy Hemorrhagic conditions Osteomyelitis Pregnancy Pacemaker Recently radiated tissue | Appears to have effect on short-term pain relief and functional improvement Three to four times per day |
| Acupuncture45 | Acute strokes Altered mental status Bleeding disorder or on blood thinners Pregnancy Seizure disorder Sepsis Unexplained red flag symptoms | One or two times per month |
Note: Each intervention listed has mild to moderate benefit.
Studies on back pain treatment support the benefit of early patient education focusing on two issues: (1) the importance of remaining physically active and avoiding bed rest; and (2) setting expectations for a positive treatment response because this may help improve outcomes.36,46
EXERCISE THERAPY
Exercise therapy is beneficial in the primary prevention of chronic low back pain and improves symptoms. Studies suggest that exercise therapy, including walking, aerobics, stretching, Pilates, yoga, tai chi, core strengthening, and spinal stabilization have potential benefit.32,47 There are no data to support the benefit of one exercise modality over another.
PHYSICAL THERAPY
Physical therapy implemented during the early phases of chronic low back pain is associated with a reduction in the need for advanced imaging, opioid use, and invasive therapies.48–51 Physical therapy interventions, including spinal stabilization exercises (examples can be found at https://orthoinfo.aaos.org/globalassets/pdfs/2017-rehab_spine.pdf), may decrease recurrent pain, medication use, and the need for health care services.32
BEHAVIORAL COUNSELING
Depression and anxiety can increase the progression to disability.52,53 Cognitive behavior therapy is a counseling technique that helps a patient think and react differently when experiencing pain. Evidence demonstrates that compared with no treatment or other guideline-based treatments, cognitive behavior therapy leads to better long-term improvement in pain intensity, disability, and quality of life.39,54
In one randomized controlled trial, mindfulness-based stress reduction and cognitive behavior therapy were more effective in the improvement of pain and functional limitation at 26 weeks compared with the usual care of physical therapy, education, and medical treatment.53 Mindfulness-based stress reduction and cognitive bahvior therapy have equivalent outcomes compared with each other.39
MULTIDISCIPLINARY BIOPSYCHOSOCIAL REHABILITATION
Multidisciplinary biopsychosocial rehabilitation was developed with the intention of addressing multiple factors that worsen chronic low back pain outcomes. This intervention involves a variety of modalities, including physical therapy, education, and behavioral components, that are often coordinated by a primary care physician.55 A Cochrane review found evidence that patients receiving multidisciplinary biopsychosocial rehabilitation experience less pain and improved function in the long-term.56 However, most studies in the Cochrane review were conducted in other countries with behavioral resources that may not be comparable with those available in the United States. There is no consensus about the definition of a multidisciplinary treatment.
MANUAL THERAPIES
Approximately 50% of patients with chronic low back pain seek spinal manipulation.57 There is evidence that it results in small improvements in pain and function.22,58–60 A meta-analysis of 47 randomized controlled trials involving 9,211 patients found that spinal manipulation outcomes were comparable, but not superior, to other recommended therapies.60
ACUPUNCTURE
There is also evidence that supports the use of acupuncture. A 2020 Cochrane review found that, although acupuncture did not provide significant benefit in the short-term (i.e., immediately after treatment), there was improvement in function and pain in the intermediate term (i.e., within seven days) compared with no treatment.61
DRY NEEDLING
A meta-analysis of dry needling showed that there was improvement in pain in short-term follow-up and was more effective for pain relief than other treatments. There was no effect on disability.62
TRANSCUTANEOUS ELECTRICAL NERVE STIMULATION
The use of transcutaneous electrical nerve stimulation for chronic low back pain is controversial because studies show mixed evidence regarding its effectiveness. Two comprehensive meta-analyses of transcutaneous electrical nerve stimulation demonstrated that there was pain reduction and improvement in short-term functional disability.63,64 Another report evaluated 169 reviews and 49 meta-analyses and found mixed results but concluded that there is likely some benefit.65
OTHER THERAPIES
Other nonpharmacologic therapies, such as traction, lumbar supports, and back school, are sometimes recommended for the treatment of chronic low back pain. However, study results are mixed and evidence is insufficient to definitively support the effectiveness of these therapies.47,66
Pharmacologic Treatment
ANTI-INFLAMMATORIES AND ANALGESICS
Nonsteroidal anti-inflammatory drugs are considered the best initial pharmacologic treatment for chronic low back pain.36,46 There is evidence that nonsteroidal anti-inflammatory drugs are more effective than placebo for improving pain and disability.22,67–69 There is no good evidence, however, that any particular nonsteroidal anti-inflammatory drug is superior to others.22,67 There is insufficient evidence to recommend the use of acetaminophen for chronic low back pain.69–71
ANTIDEPRESSANTS
A systematic review demonstrated that there was no benefit from tricyclic antidepressants or selective serotonin reuptake inhibitors compared with placebo for treatment of chronic low back pain.70 However, there is moderate evidence that duloxetine (Cymbalta), a serotonin-norepinephrine reuptake inhibitor, provides a small improvement in pain compared with placebo over a four-month period. Adverse effects can potentially lead to discontinuation of the medication.32,72,73
MUSCLE RELAXANTS AND SEDATIVE HYPNOTICS
Muscle relaxants (e.g., carisoprodol, tizanidine, cyclobenzaprine, thiocolchicoside [not available in the United States], orphenadrine, metaxalone, methocarbamol, baclofen) demonstrate that there is no benefit compared with controls for pain, disability, and acceptability.24
Studies also demonstrate that there is no benefit with benzodiazepines vs. placebo for chronic low back pain, and there is a significant risk of harm.25,69 Studies of medications for improving sleep found that there is an unlikely clinical benefit in patients with chronic low back pain.74
CORTICOSTEROIDS
Oral systemic corticosteroids have not been shown to be effective for chronic low back pain, with or without radiculopathy.22 There was no benefit in pain control with corticosteroids in patients with chronic low back pain or spinal stenosis in the long-term (i.e., 12 months or greater).75
Epidural corticosteroid injections are not effective for providing long-term relief of disability or pain.76 They may provide a slight reduction in pain and disability in the short-term for patients with radicular pain based on limited data.76
ANTICONVULSANTS
Anticonvulsants are often used off-label for radicular back pain, such as sciatica from spinal stenosis. However, recent moderate- to high-quality evidence suggests that anticonvulsants, such as topiramate, gabapentin, and pregabalin (Lyrica), are not effective treatments for chronic low back pain.77
OPIOIDS
For short-term use, there is low-quality evidence that opioids may have a small, clinically significant benefit for pain and function. However, the use of these medications is associated with adverse effects and increased risk of harm compared with nonopioid medications. Therefore, multiple professional organizations recommend against prescribing opioids for chronic low back pain before a comprehensive evaluation, trial of alternative medications and treatments, and discussion about the risks of opioid therapy.22,78,79
Long-term opioid use has been shown to be less effective than nonopioids in reducing pain and improving function or disability. Long-term opioid therapy, including tramadol, should be avoided due to the risks of abuse or dependence and other adverse effects.22
CANNABIS
Evidence regarding the effectiveness of cannabis for chronic low back pain is inconclusive. There is a limited number of randomized controlled trials, and further studies are needed to assess the benefits and risks.80
Procedural Intervention
RADIOFREQUENCY DENERVATION AND SPINAL CORD STIMULATION
Radiofrequency denervation uses heat to destroy nerves that cause pain. It may be associated with a small increase in short-term pain relief, but a Cochrane review of 23 randomized controlled trials found no high-quality evidence that it is an effective treatment for chronic low back pain.81,82
Spinal cord stimulation is a surgical intervention that uses an implantable device to regulate pain through electrical signals. A Cochrane review suggests that this therapy is not beneficial for low back pain or worth the cost.83
SURGERY
Most patients with chronic low back pain do not need surgery.5 Surgical consultation may be considered for patients with persistent functional disabilities, pain from progressive spinal stenosis with nerve impingement, worsening spondylolisthesis, or a herniated disk.
For patients with unilateral sciatica due to lumbar disk herniation lasting at least four months and who have consistent imaging and physical examination findings, surgery results in greater improvement in pain, disability, and quality of life at six months vs. conservative treatment.26
Spinal fusion surgery for degenerative, nonradicular chronic low back pain is controversial. Randomized trials show no definitive benefit compared with a multidisciplinary, nonsurgical approach, including rehabilitation.84,85
Prevention
Preventing the transition from acute low back pain to chronic low back pain is important. Physicians often underestimate the rate of progression to chronic low back pain, which can be as high as 32% at six months.6 Several screening tools are available to assess the risk of progression, including the PICKUP score (https://www.evidencio.com/models/show/1119), short form of the Örebro Musculoskeletal Pain Screening Questionnaire (https://orthotoolkit.com/ompsq-sf), and STarT Back calculator (https://startback.hfac.keele.ac.uk/training/resources/startback-online).36
When there is an increased risk of progression to chronic low back pain, guidance about targeted treatment strategies based on risk category is available at https://www.youtube.com/watch?v=tHMJf74buW4. [corrected] This approach appears to have more effective outcomes than the usual care of physical therapy, back exercises, and medication treatment.5,36,86–89
A National Institutes of Health study of 5,233 patients at 77 primary care sites in the United States found that early implementation of the STarT Back program was associated with decreased progression to chronic low back pain, reduced pain, improved function and quality of life, and better overall treatment satisfaction.6,56 Data showed that there were 50% fewer work absences, a decrease in unnecessary referrals to physical therapy, less use of nonsteroidal anti-inflammatory drugs, and an overall reduction in health care use.90
This article updates previous articles on this topic by Herndon, et al.,20 and Last and Hulbert.91
Data Sources: A literature search was performed using the key words chronic low back pain. Sources included PubMed; Cochrane Database; Essential Evidence Plus, including POEMs; and Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain: A Clinical Practice Guideline from the American College of Physicians. We used references from the previous American Family Physician articles on chronic low back pain from 2015 and 2000. Search dates: January 14, 2023, and January 26, 2024.
