Case Scenario
My 74-year-old patient, V.P., who has a history of osteoarthritis and hypertension, reports hearing loss during a wellness visit. V.P. works in customer service taking telephone calls but is becoming fatigued trying to hear customers on the phone and is concerned that hearing loss may be affecting their ability to remember details at work. On further questioning, V.P. reports slowly progressive, bilateral hearing loss without ear pain, drainage, tinnitus, or vertigo. Examination shows normal-appearing external ears without injury or deformity, clear canals bilaterally, and normal-appearing tympanic membranes.
V.P. also states that family members have been complaining about the excessive volume of the television at home. V.P. has taken a home hearing test, which shows evidence of bilateral hearing loss. My patient is concerned about the cost of prescription hearing aids and asks whether less expensive, over-the-counter (OTC) hearing aids could help or whether it would be better to see a specialist. Is my patient a suitable candidate for OTC hearing aids? What can I offer my patient to help them make the best choice?
Commentary
Helen Keller famously stated that deafness separates us from people. Reports of perceived hearing loss should be taken seriously and explored with patients. Of American adults 75 years or older, 50% have perceived disabling hearing loss; fewer than one-third of patients 70 years and older who could benefit from hearing aids have ever used them.1 Hearing loss is invisible, often unacknowledged or denied, and is a potentially modifiable risk factor for dementia.2,3 Hearing loss is strongly tied to social determinants of health and is associated with geriatric frailty, depression, disability, social isolation, unmet medical needs, and increased health care costs. In primary care, patients are not routinely screened for hearing loss, and the issue is not often addressed.4–6 The average age at which people first use hearing aids is 80 years, with approximately 10 years lapsing between identified hearing loss and use of amplification.7 Traditional Medicare Part B does not cover hearing examinations or hearing aids but does pay for hearing tests related to treating conditions other than hearing loss (e.g., memory loss). Some state Medicaid programs and more than 90% of Medicare Advantage programs pay for hearing assessments and amplification, but regulations and coverage vary among programs.8,9
With the U.S. Food and Drug Administration (FDA) approval of OTC hearing aids in August 2022, physicians will likely have a larger role in guiding patients interested in acquiring hearing aids.10 OTC hearing aids received approval after determination that safety and effectiveness were well established and that the benefits of a regulated market for hearing aids outweighed any theoretical risks. This position is supported by the Hearing Loss Association of America as an initiative to destigmatize hearing loss and support affordable hearing care services and technology innovation for the more than 48 million Americans who experience hearing loss.11
HEARING ASSESSMENT
OTC hearing aids are appropriate for adults 18 years and older who have self-perceived, mild to moderate hearing loss and who have no concerning conditions that require a formal hearing evaluation. Symptoms warranting medical evaluation, including warning symptoms as defined by the FDA (e.g., sudden-onset hearing loss, pain, vertigo, unilateral hearing loss), should be assessed by a primary care physician. Table 1 details signs and symptoms of hearing loss, including additional indications for medical assessment.10 An article containing a detailed differential diagnosis and information on the assessment of hearing loss is available in American Family Physician.12
TABLE 1. Signs and Symptoms of Hearing Loss
| Mild to moderate |
| Asking others to speak louder, more slowly, or more clearly or to repeat what was said |
| Becoming fatigued with prolonged listening |
| Difficulty hearing in a group |
| Difficulty hearing in a noisy area |
| Difficulty hearing while on the phone |
| Muffling of speech and other sounds |
| Radio, music, or television volume is louder than preferred by others |
| Severe |
| Trouble hearing loud sounds |
| Trouble hearing speech in quiet places |
| Warning symptoms requiring additional evaluation |
| Asymmetrical hearing loss |
| Clear or purulent discharge or blood from ears |
| Feeling of blockage of the ear canal |
| History of excessive ear wax |
| New onset of tinnitus (hearing sound when no external sound is present) in one or both ears |
| New sensation of dizziness or vertigo |
| Pain or discomfort in the ear |
| Sudden hearing loss or acute worsening of chronic hearing loss |
Information from reference 10.
After concerning medical conditions associated with hearing loss have been ruled out, a hearing evaluation by a licensed hearing specialist/audiologist or a hearing test conducted at home is the next step. The clinical standard for hearing assessment is pure-tone audiometry to determine the severity of hearing loss and whether hearing amplification is appropriate for the patient12; however, a variety of home hearing tests are available, including online-based screening using downloadable software to a computer or smartphone or through apps with a landline phone. Home hearing testing was shown in one study to be an accurate and cost-effective method of establishing pure-tone air conduction thresholds compared with manual audiometry.13
PRESCRIPTION VS. OTC HEARING AIDS
Principal factors that guide hearing aid selection include cosmesis, sound quality, dexterity, and technologic literacy. Together, these factors affect the cost of the hearing aid. An understanding of the patient's needs and preferences can guide the physician in recommending the OTC route vs. referral to a hearing specialist. Table 2 lists types and features of OTC and prescription hearing aids.2,14–16 Additional devices are also available to assist individuals with hearing impairment, including personal sound amplification products, modified telephones, and adaptive equipment for the home (eTable A).
TABLE 2. Type and Features of Over-the-Counter and Prescription Hearing Aids
| Style* | Type of hearing loss | Size | Charging | Level of dexterity | Extra features | Disadvantages |
|---|---|---|---|---|---|---|
| Behind the ear | Almost any type (mild to profound) | Typically the largest | Some are rechargeable | Easiest to use | Volume control14,15 | — |
| In the canal, completely in the canal | Mild to moderate | Smallest and least visible type | Batteries that have a shorter life | Small batteries that can be difficult to handle | — | Often does not include extra features (e.g., volume control, directional microphones); susceptible to earwax clogging the speaker; may be too small to include telecoil option15 |
| Receiver in canal, receiver in the ear, “mini” behind the ear | Mild to severe | Typically less visible than behind-the-ear option | Rechargeable | Typically requires a good level of manual dexterity | Volume control14,16; directional microphones; may offer more natural sound quality | Susceptible to earwax clogging the speaker |
| In the ear | Moderate to severe | Full shell (i.e., fills entire ear) or half shell (i.e., fills a portion of the bowl of the ear) | Vary by manufacturer | Best for dexterity issues or difficulty handling small items | Can include volume control2,16 | — |
*—Listed in order of use for mild to most severe hearing loss.
Prescription hearing aids are acquired from a licensed hearing specialist or audiologist who will advise on the choice of hearing aid type and style. The medical hearing professional ensures proper fit and programs the device for maximum hearing and comfort. Professional support often includes instructions on placement, follow-up adjustments, cleaning, and maintenance.17 Prescription hearing aids may be better for patients who lack technologic skill or who have limited support at home. Prescription hearing aids are the most expensive option, with potential out-of-pocket costs ranging from $1,000 to $6,000, and they often require multiple visits to a hearing professional's office.17
If an OTC hearing aid is chosen after a hearing assessment, different sound adjustment customization options are available, including preset and self-fitting and assorted styles and features (e.g., behind the ear, in the ear). Additional features may raise the price of the device without providing meaningful perceived benefit. In-the-ear aids are smaller but may be harder to manipulate if dexterity is a concern. The behind-the-ear style provides superior sound quality and filters background noise more effectively than in-the-ear styles.17 A patient who is technologically savvy might prefer hearing aids that are capable of pairing to a smartphone and connecting to various Bluetooth devices. A patient who enjoys the theater or going to church may appreciate the sound qualities of a device equipped with a telecoil (a process of filtering extraneous sounds). Table 3 lists technologic features of various hearing aids.16,18–22
TABLE 3. Technologic Features of Over-the-Counter and Prescription Hearing Aids
| Advanced microphone setting (directional microphones) Improve pickup of sounds in front of the user with some reduction of sounds from other directions, which can improve the ability to hear in the presence of background noise18,19 |
| Automatic and manual noise level Newer hearing aids can sample the listening environment and automatically adjust volume and microphone settings to optimize speech understanding and comfort20 |
| Digital noise reduction Present in all devices to reduce certain noises (e.g., wind)16,18 |
| Feedback suppression Helps prevent the production of a squealing sound18,21 |
| Multiple programmed settings Some hearing aids can store several preprogrammed settings to aid with various listening needs and environments16 |
| Rechargeable batteries Allow for easier maintenance because batteries do not need to be removed and changed; can be helpful for those with dexterity issues16 |
| Smartphone capabilities Newer hearing aids allow for connection to smartphones to adjust volume and listening profiles on the hearing aids; some companies offer remote adjustments via their company's smartphone app18 |
| Telecoil (T-coil) Allows use of hearing aid with other devices or in facilities (e.g., churches, theaters) that are equipped with specialized hearing assistive technology (i.e., hearing loop) to improve the sound quality (e.g., of a speaker, play, movie); telecoils make it easier to hear when talking on a telecoil-compatible phone by reducing environmental sounds and improving the sound of the person speaking16,18 |
| Tinnitus masking Most hearing aids can adjust the volume of external noise to the point that it covers or masks the sound of tinnitus, which helps the brain focus on outside or ambient noises rather than the tinnitus22 |
| Wireless connectivity (Bluetooth) Newer hearing aids can connect with some Bluetooth-capable devices (e.g., cellphones, computers, televisions); some hearing aids require an intermediary device to pick up the secondary device and send the signal to the hearing aid16 |
Note: Features pertain to prescription hearing aids; features for over-the-counter hearing aids vary.
One type of OTC hearing aid is referred to as “self-fitting.” This type of device typically has automated fitting, the ability to operate without clinical assistance, and user options to adjust settings using manual controls or software. One study found that self-fitting hearing aids with remote support had comparable outcomes to prescription-fitted devices after six weeks for self-reported global benefit.23 This type of OTC aid is customizable and requires the most technologic skill of users. Self-fitting hearing aids must be set up and regulated via a smartphone app.
Preset OTC hearing aids can also be purchased in retail stores or online. They give the consumer the choice of a few audio program settings and are less complicated to set up and use. These hearing aids are less easily customized to specific hearing needs than alternative devices; however, one study suggests that a few selected presets are capable of meeting most hearing needs in 67% of older adults with mild to moderate hearing loss.24 The FDA does not monitor preset hearing aids as closely as self-fitting aids.17
When discussing the use of OTC hearing aids with patients, it is important to ensure that they understand the customer support provided with the device. The hearing aid should have an allowable trial period of at least one month, a well-documented return policy, and an appropriate warranty.17 Figure 1 proposes an approach to caring for a patient with hearing loss.25
FIGURE 1.
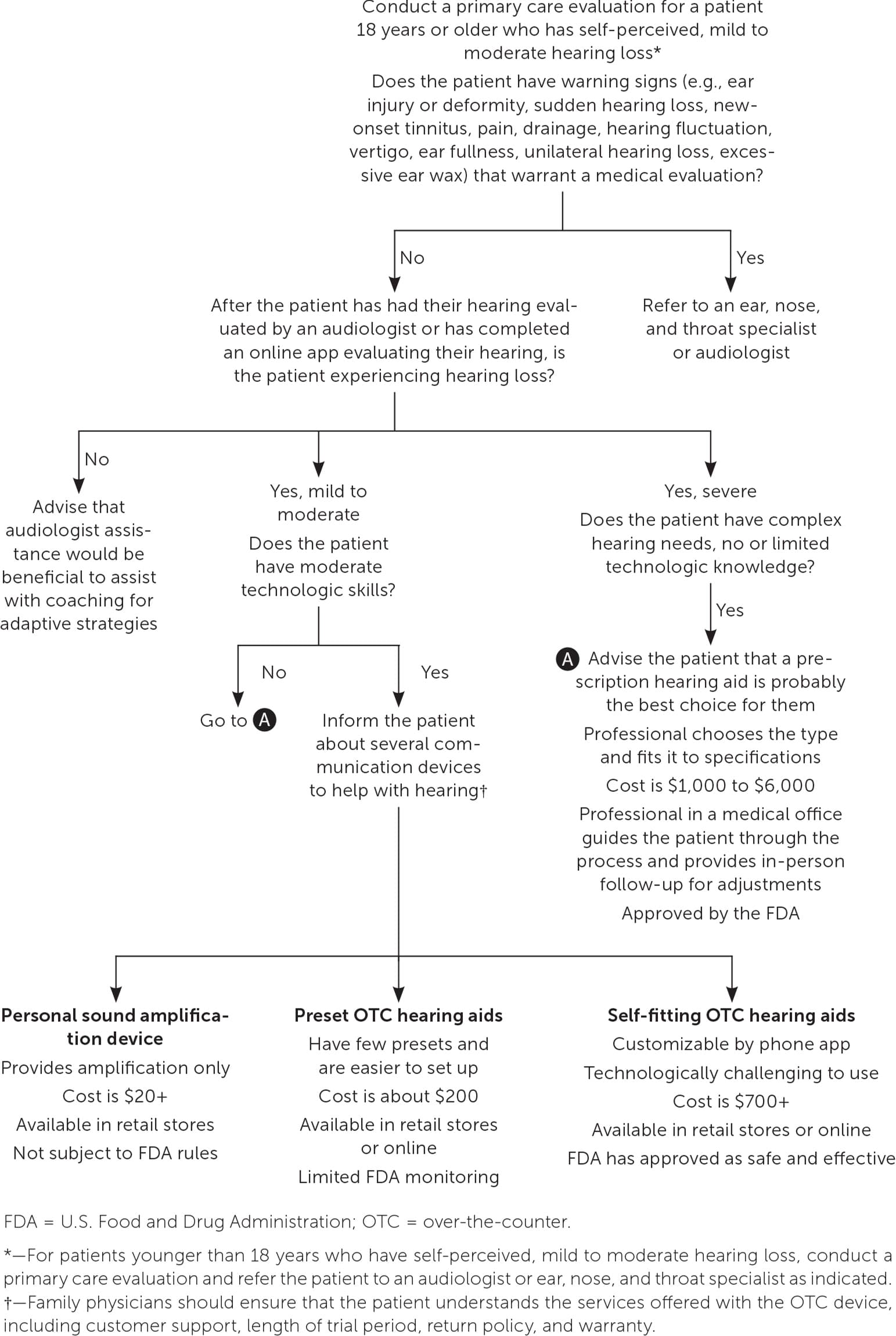
Approach to caring for a patient experiencing hearing loss.
Information from reference 25.
OTHER COMMUNICATION SOLUTIONS
State Technology Assistance Programs can help individuals who are deaf and hearing-impaired and their families or caregivers; for example, the state of Virginia offers telecommunication equipment and assistive technology to qualified applicants.26 Specialized telecommunication equipment is available to assist patients who are deaf, hard of hearing, deaf and blind, or for those with difficulty speaking26 (eTable A). Personal sound amplification products, also called hearables, are approved by the FDA as electronic devices but not as medical devices. The products are intended for people with normal hearing and are designed to enhance sound during certain recreational activities, such as watching television and birdwatching.27
eTABLE A Communication Options for Patients With Hearing Loss
| Alarm clocks with bed shaker, flashing lights, loud ringers |
| Alert patients to calls, visitors, or emergencies |
| Doorbells |
| Alert patients using flashing lights or loud chime sound |
| Personal sound amplification products |
| Use amplifiers to provide sounds derived from voice, television, or radio directed to a headset |
| Telephone features |
| Amplified: amplifies ringer and speaker's voice |
| Captioned: provides simultaneous conversation and captions on a display in real time |
| Hearing carryover: allows an individual to type a response (typically for those who have difficulty speaking) |
| Ringer: uses flashing lights or loud chime sounds to alert patient |
| Text: allows an individual to type comments on a keyboard and to read responses on a text screen |
| Voice carryover: allows an individual to speak directly on the phone or read responses on the display; does not allow voice carryover user to hear the voice of the other party |
Information from Virginia Department for the Deaf and Hard of Hearing. Technology Assistance Program (TAP). Accessed August 6, 2023. https://www.vddhh.virginia.gov/equipment.htm
Case Resolution
Your patient wants and needs better hearing. No warning symptoms or concerns are noted on V.P.'s history or examination, and their hearing loss appears to fall in the mild to moderate category. A formal audiology assessment may be covered by Medicare because V.P. has noted memory changes associated with their hearing deficit. Factors to consider include V.P.'s manual dexterity and comfort with technology, including daily use of a smartphone and the ability to easily access information on the internet. Accounting for V.P.'s concerns about cost, quality, and agility, a behind-the-ear, rechargeable, preset, OTC hearing aid could be recommended.
