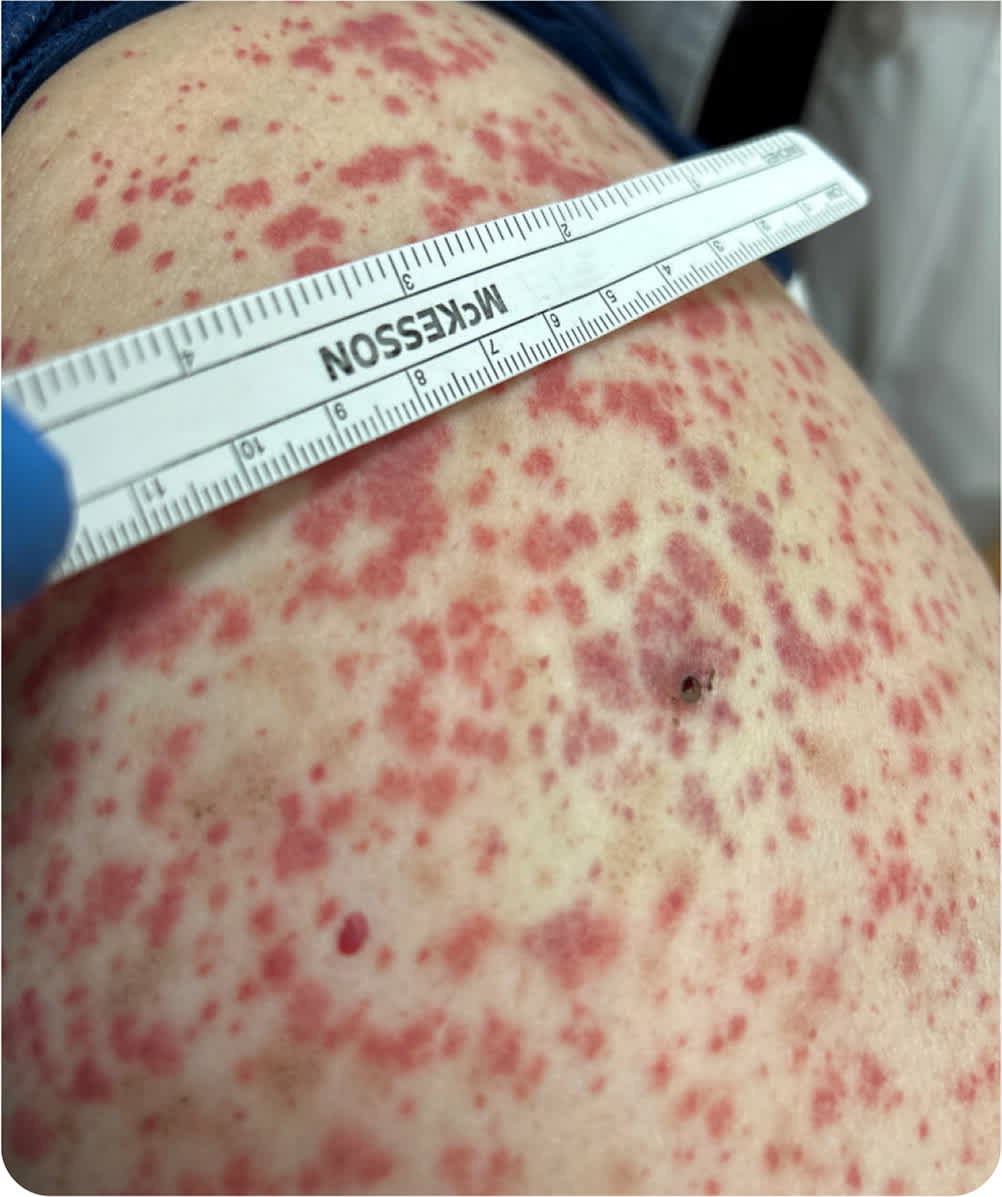
A 57-year-old woman who had a history of osteoarthritis presented with a nonpruritic rash associated with paresthesia, myalgia, and worsening joint pain. The rash began on the soles of her feet and ascended toward her trunk. Her symptoms began 48 hours after starting atorvastatin and empagliflozin (Jardiance) for metabolic syndrome.
Examination revealed tender, nonblanching, palpable purpura extending from the bilateral lower extremities to the proximal thigh (Figure 1). A complete blood count, comprehensive metabolic panel, antinuclear antibody panel, and antineutrophil cytoplasmic antibody test were all unremarkable. Urinalysis was significant for proteinuria and hematuria. Punch biopsy of a lesion showed a predominantly neutrophilic infiltrate in the dermis with fibrinoid necrosis of wall vessels.
FIGURE 1
The patient later presented to the emergency department with acute abdominal pain; computed tomography showed inflammation of the terminal ileum.
Question
Based on the patient's history and physical examination, which one of the following is the most likely diagnosis?
- A. Cutaneous small vessel vasculitis.
- B. Eosinophilic granulomatosis with polyangiitis.
- C. Immunoglobulin A vasculitis.
- D. Polyarteritis nodosa.
Discussion
The answer is C: immunoglobulin A vasculitis, previously known as Henoch-Schönlein purpura. This is an inflammatory disorder of the blood vessels that results in damage primarily to the skin, joints, intestines, and kidneys.1 It is the most common systemic vasculitis in children, but it can occur in adults, with an estimated incidence of 3.4 to 14.3 cases per million.2
Children and adults with immunoglobulin A vasculitis have similar clinical manifestations. Most present with a skin rash, abdominal pain, and hematuria. One-fourth of adults present with joint involvement. Medications are most likely to be the precipitating factor in adults.3 Biopsy showing pathology consistent with leukocytoclastic vasculitis confirms the diagnosis. Positive pathologic and immunologic findings on skin biopsy are highly sensitive for the diagnosis 24 to 48 hours after lesion onset.4
This patient met three of the four American College of Rheumatology diagnostic criteria for immunoglobulin A vasculitis (palpable purpura, acute abdominal pain, and renal involvement; the fourth criterion is age younger than 20 years).5 She met all of the European Alliance of Associations for Rheumatology adult criteria (palpable purpura, abdominal pain, arthritis, kidney involvement, leukocytoclastic vasculitis, and proliferative glomerulonephritis).6 Biopsy did not show immunoglobulin A deposits, but this did not rule out immunoglobulin A vasculitis. Her renal function deteriorated, and renal biopsy confirmed immunoglobulin A glomerulonephritis.
Systemic steroids may help shorten the duration of symptoms, but they do not slow renal progression.7 More than one-half of patients with renal involvement develop progressive or relapsing immunoglobulin A vasculitis.8 There may also be an association with malignancy.9
Cutaneous small vessel vasculitis is localized to the skin, usually on the lower legs, and presents with palpable purpura. It is associated with exposure to certain medications, including antibiotics, thiazides, phenytoin, and nonsteroidal anti-inflammatory drugs; infections, such as streptococci and hepatitis; and connective tissue disorders, such as systemic lupus erythematosus and rheumatoid arthritis. The condition is generally benign and resolves after days to weeks without treatment.10
Eosinophilic granulomatosis with polyangiitis, previously known as Churg-Strauss syndrome, affects small- and medium-sized arteries. There are three phases of the disease: prodromal (asthma, eczema, or rhinitis), eosinophilic (eosinophils infiltrating in multiple organs), and vasculitic (affecting the vascular system with nonspecific constitutional signs).11 Patients often have an accumulation of eosinophils, typically seen on blood smear testing or biopsy of a blood vessel.
Polyarteritis nodosa is a systemic, segmental, transmural inflammation of medium-sized muscular arteries and small-sized arteries. It commonly affects men older than 50 years. Skin and neurologic involvement occur in approximately 49% and 70% of patients, respectively. It is associated with hepatitis B, hepatitis C, and hairy cell leukemia.12 The condition typically does not feature antineutrophilic cytoplasmic antibodies.
SUMMARY TABLE
| Condition | Characteristics |
|---|---|
| Cutaneous small vessel vasculitis | Palpable purpura localized to the skin, usually on the lower legs; associated with exposure to certain medications (e.g., antibiotics, thiazides, phenytoin, nonsteroidal anti-inflammatory drugs), infections (e.g., streptococci, hepatitis), and connective tissue disorders (e.g., systemic lupus erythematosus, rheumatoid arthritis) |
| Eosinophilic granulomatosis with polyangiitis | Affects small- and medium-sized arteries; three phases: prodromal (asthma, eczema, or rhinitis), eosinophilic (eosinophils infiltrating in multiple organs), and vasculitic (affecting the vascular system with nonspecific constitutional signs); accumulation of eosinophils is typically seen on blood smear testing or biopsy |
| Immunoglobulin A vasculitis | Skin rash, abdominal pain, joint pain, and hematuria; symptoms similar in children and adults; medications are most likely to be precipitating factor in adults; condition is often progressive or relapsing in patients with renal involvement |
| Polyarteritis nodosa | Systemic, segmental, and transmural inflammation of medium-sized muscular arteries and small-sized arteries; commonly affects men older than 50 years; associated with hepatitis B, hepatitis C, and hairy cell leukemia |
