
Introduction
Eosinophilic esophagitis (EoE) is a chronic, allergen-induced, immune-mediated disease characterized by esophageal dysfunction and eosinophil-predominant esophageal infiltration.1,2 EoE has only recently been recognized as a distinct clinical entity, with its incidence and prevalence rising sharply over the past two decades.1
EoE affects patients across all age groups and occurs more frequently in males. Earlier assumptions that EoE primarily occurs in White individuals likely reflect bias in study participation and reporting, rather than true biologic differences.3,4
Patients with EoE are often found to have one or more atopic comorbidities.5 Familial clustering supports a contribution from genetic susceptibility, but twin and family studies show that shared environmental factors play a far greater role than genetics in disease development.6,7
Learning Objective(s)
- Explain the role of type 2 inflammation in the disease development and treatment considerations for eosinophilic esophagitis (EoE).
- Assess signs and symptoms of EoE that should prompt further clinical investigation.
- Apply evidence-based strategies to efficiently identify EoE in affected patients.
- Summarize strategies for optimizing referrals and follow-up care management in primary care for patients with EoE.
Pathophysiology and Immunopathology of EoE
EoE belongs to the spectrum of type 2 inflammatory diseases, which includes asthma, allergic rhinitis, chronic rhinosinusitis, atopic dermatitis, and food and drug allergies.8 These disorders share common immune mechanisms,9–11 and patients with multiple allergic diseases and symptoms of esophageal dysfunction warrant heightened suspicion for EoE.9
Key Cellular and Cytokine Pathways
In a genetically predisposed individual, barrier dysfunction in the esophageal epithelium allows penetration of food and aeroallergens, which trigger epithelial cells to release alarmins, initiating the inflammatory cascade.8,11,12 These alarmins activate type 2 immune cells,8,9 which release cytokines that weaken barrier integrity, promote tissue remodeling, and recruit eosinophils, a defining feature of EoE.13,14 Over time, this inflammatory state can give way to collagen deposition and esophageal fibrostenotic disease, with esophageal rings and strictures as potential complications.15
Clinical Presentation and Diagnosis of EoE
EoE manifests clinically through diverse symptoms that vary by age and can evolve over time (Table).16
Table. Spectrum of presenting symptoms of eosinophilic esophagitis across the lifespan16
| Symptom Type | Age Group | ||
|---|---|---|---|
| Infants/Young Children | Older Children/Adolescents | Adults | |
| Feeding/Eating | Feeding aversion, delayed feeding skills, texture preferences | Preference for soft foods, avoidance of solids, meal-time anxiety | |
| GI Symptoms | Vomiting, irritability, abdominal pain | Abdominal pain, vomiting, heartburn | Chest or upper abdominal pain, heartburn |
| Obstructive Events | Rare in this age group | Dysphagia, coughing and gagging, food impaction | Dysphagia, food impaction |
Abbreviation: GI, gastrointestinal.
Adapted from: Horwitz A, Yunus S. Med Clin North Am. 2024;108:733–745.
The hallmark feature of EoE is dysphagia, and it is essential that primary care physicians (PCPs) elicit a careful history of symptoms of esophageal dysfunction, including dietary avoidance and modification behaviors, as patients frequently adopt subtle coping strategies (Figure).2
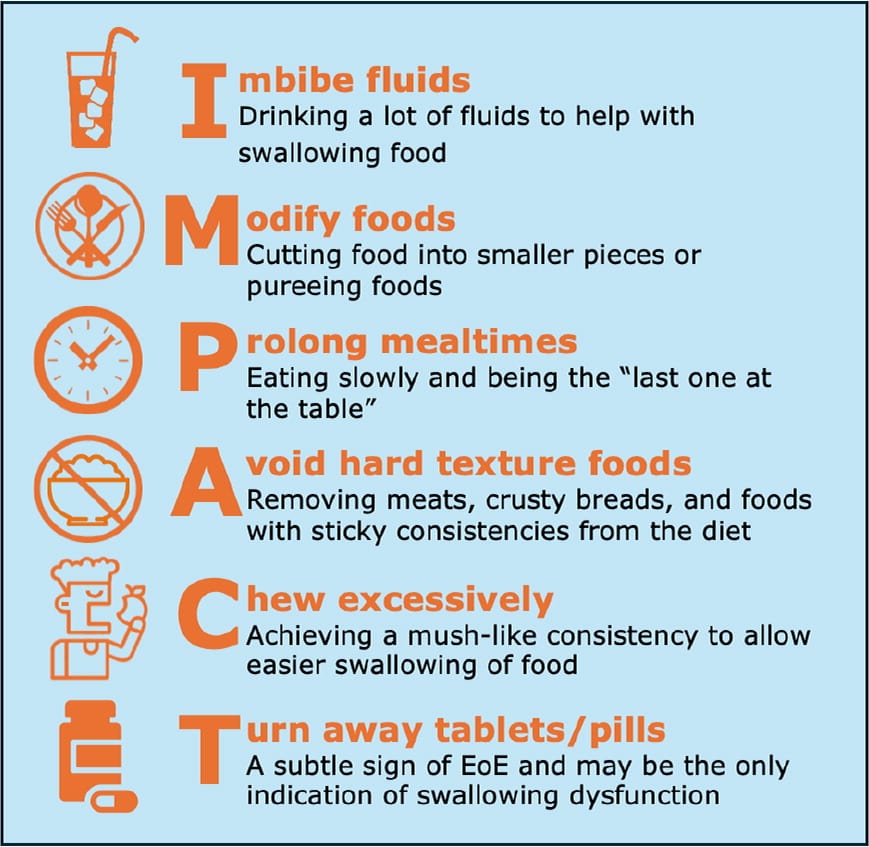
Figure. IMPACT behaviors to assess while taking a dysphagia history2
Adapted from: Dellon ES, Muir AB, Katzka DA, et al. Am J Gastroenterol. 2025;120:31–59.
Chest pain and acid reflux are common but nonspecific, often leading to initial treatment for other conditions like gastroesophageal reflux disease (GERD). GERD and EoE are not mutually exclusive. In fact, they are likely interdependent, with GERD furthering epithelial barrier dysfunction, and EoE leading to secondary reflux due to esophageal compliance and dysmotility.17 Suspicion for EoE should lead PCPs to refer patients to a gastroenterologist (see sidebar: Role of the PCP in Suspected EoE).18
Diagnostic Workup
Diagnosis requires symptoms of esophageal dysfunction, at least 15 eosinophils per high-power field (eos/hpf) on esophageal biopsy, and exclusion of other causes of esophageal eosinophilia. Since eosinophilic inflammation is often patchy, current guidelines recommend at least six biopsies from at least two esophageal levels, regardless of esophageal appearance.2,19
Endoscopic assessment should also document characteristic findings using the EoE Endoscopic Reference Score (EREFS), a validated system shown to distinguish EoE from non-EoE disorders with high accuracy in both children and adults. EREFS scores Edema, Rings, Exudates, Furrows, and Strictures on a total scale of 0 to 9, based on the most severely affected esophageal region.2
Consequences of Diagnostic Delay
Diagnosis typically occurs 1.2 to 3.5 years after symptom onset in children and 3 to 8 years in adults. Inflammatory features (edema, furrows, and exudates) appear earlier, whereas fibrostenotic features (rings and strictures) emerge later. Longer diagnostic delays correlate with more advanced fibrosis.22 In children, delay can cause feeding-related behavioral issues or failure to thrive.23 Early recognition of persistent dysphagia and timely endoscopic referral help interrupt disease progression.
Management of EoE
Patients with EoE often require a multidisciplinary team approach, including gastroenterologists, allergists, pathologists, dietitians, feeding therapists, mental health professionals, and/or specialty pharmacists, depending on the patient's individual needs.23 Treatment goals include minimizing diagnostic delay, ensuring effective therapy with minimal adverse effects (AEs), monitoring well-being, preventing malnutrition, and managing atopic comorbidities.23
PCPs play a distinct role in sustaining continuity of care. Through long-standing relationships and frequent contact with patients, PCPs are uniquely positioned to recognize persistent or unresponsive symptoms, review treatment options, reinforce adherence, and facilitate specialty follow-ups.11,18
Dietary Therapy
Dietary elimination is a cornerstone of EoE management, based on the principle that avoiding trigger foods can reduce esophageal inflammation and achieve disease remission.
Elemental diets use amino-acid–based hypoallergenic formulas lacking food allergens and achieve high histologic response rates (>90%), but poor palatability, cost, and adherence challenges limit use to infants or severe refractory cases.2
Empiric food elimination diets (FEDs) eliminate specific foods or food groups for 6 to 8 weeks, followed by systematic reintroduction with endoscopic assessment.2 Traditional “step-down” approaches start with broad restrictions and reintroduce foods sequentially. “Step-up” approaches begin with fewer restrictions, expanding restrictions only if inflammation persists.
The six-food elimination diet (6FED)—removing milk, wheat, soy, egg, tree nuts/peanuts, and fish/shellfish—achieves histologic remission in up to 70% of patients but is highly restrictive and requires multiple endoscopies.2,15,24
The 2FED—removing milk and wheat, the most common triggers— achieves remission in a substantial proportion of patients, with escalation to a 4FED or 6FED, if needed.2 Even the 1FED—milk avoidance alone—has shown similar impacts, compared with 4FED.25,26
The optimal diet is one that patients can sustain, ideally with dietitian guidance to maintain balanced nutrition, as about half of patients cannot maintain dietary restrictions on a long-term basis.2,15,24 PCPs should monitor for nutritional adequacy, particularly evaluating growth in children and nutrient deficiencies. Additionally, PCPs should assess adherence, identify new or worsening dysphagia or feeding difficulties, and encourage gastroenterology and dietitian follow-up for struggling patients.
Pharmacologic Management
The key role for PCPs is monitoring for side effects, asking about adherence, and reinforcing the importance of follow-up endoscopy with biopsies to confirm disease control. Three main classes of medications are used in EoE: proton pump inhibitors (PPIs), swallowed topical corticosteroids (STCs), and biologics.
Proton pump inhibitors
PPIs are a first-line treatment option for EoE. Their benefit extends beyond acid suppression—they reduce secretion of the cytokine eotaxin-3, improve epithelial barrier function, and help restore normal esophageal biology. This explains why PPIs can be effective even when GERD symptoms are absent, a point worth clarifying with patients to support adherence.2,18
The American College of Gastroenterology (ACG) guidelines recommend “high-dose” therapy—typically double the standard dose for GERD—once daily or in two divided doses.2 After remission, dosing may be reduced, though some patients relapse and require re-escalation.2 PCPs should monitor for flare-ups, such as recurrent dysphagia.
Long-term safety data are generally reassuring. However, there is an increased risk of Clostridium difficile infection, so PCPs should be aware of the clinical features.27
Swallowed topical corticosteroids
STCs are also a first-line option for inducing remission in EoE. Trials consistently show histologic response rates of 60% to 70% with off-label use of topical corticosteroids formulated for asthma.2 Treatment choices were expanded when a newer formulation, budesonide oral suspension (BOS), was FDA approved in 2024 for 12 weeks of treatment in patients aged 11 years and older.28 Off-label use of asthma inhalers—fluticasone swallowed after actuation—or thickened budesonide liquid remains common. While these approaches are effective, BOS offers a standardized formulation, optimized esophageal delivery, and improved patient convenience.2,11
Unlike systemic corticosteroids, STCs act locally on the esophageal mucosa with minimal systemic absorption, which explains their favorable safety profile. The main AE of concern, reported in fewer than 5% of patients using BOS, is oral or esophageal candidiasis, which is usually mild and treatable with antifungals. Rare cases of adrenal suppression have been reported, particularly with long-term or multiple steroid exposures.2
Biologics
Dupilumab is a monoclonal antibody that blocks IL-4 and IL-13, key type 2 inflammatory cytokines.2 FDA approval came in 2022 for adults and adolescents aged 12 years and older with EoE,29 expanded in 2024 to include children aged 1 year and older weighing at least 15 kg.30
Dupilumab is typically considered when patients do not respond to PPIs or STCs18 and should be considered for early use in patients with moderate to severe asthma or atopic dermatitis.2 Dosing varies by age and weight. Dupilumab is generally well tolerated, with the most common AE being injection-site reactions; others include upper respiratory infections, arthralgia, and herpes viral infection.2
Type 2 inflammatory pathways driving EoE are shared across other allergic diseases, explaining why targeted treatments can be effective across multiple conditions. For example, dupilumab's approved indications include asthma, atopic dermatitis, and chronic rhinosinusitis with nasal polyps. For patients with multiple atopies, the PCP's role centers on maintaining a complete medication list to identify overlap, minimize redundancy, and monitor for potential interactions.
Psychosocial and Mental Health Burden of EoE
EoE places a substantial psychosocial burden on patients. In pediatric patients, feeding difficulties, prolonged mealtimes, and fear of choking can disrupt normal growth, sleep, and participation in school and social activities, and these challenges often extend to caregivers.21
In adults, chronic dysphagia and dietary restrictions are linked with anxiety, depression, and reduced quality of life, with young adults at the highest risk.30 Some patients develop extreme restrictive eating behaviors from fear of symptoms or complications. This can interfere with nutrition, social functioning, and adherence, creating a cycle where emotional distress worsens disease management.30
PCPs' long-term relationships with patients and families position them well to notice these psychosocial impacts during routine visits. Routine screening questions about stress at mealtimes, changes in eating behaviors, or signs of anxiety and depression can help identify when patients may need additional support or referral to mental health services.30
Long-Term Monitoring and Follow-Up
EoE almost always recurs when treatment is stopped, requiring ongoing monitoring. The goal is confirming disease control across symptoms, endoscopic findings, and histology; active inflammation may persist, despite symptomatic improvement.2
Guidelines recommend follow-up endoscopy with biopsies 2 to 6 months after initiating or changing therapy. Subsequent surveillance depends on disease severity: patients with food impaction, strictures, or malnutrition may need closer follow-up, while stable patients can be monitored at longer intervals. Still, long intervals (especially 2 years or more) without endoscopic reassessment have been linked to increased risk of fibrostenotic progression.2
Role of PCPs in the Ongoing Care of the Patient With EoE
In patients with a history of impactions or strictures, PCPs should prescribe liquid, chewable, or dissolvable medication formulations to minimize obstruction risk.
PCPs play a continuing role in long-term surveillance by monitoring for symptom recurrence and any side effects, tracking growth and nutrition (particularly in children), and ensuring gastroenterology follow-up. Urgent referral is warranted for food impaction or severe dysphagia, while routine reassessment should be encouraged for milder recurrences or treatment concerns.
Role of the PCP in Suspected EoE
- Ask early: Evaluate patients with chest pain or reflux for possible EoE, especially if symptoms are recurrent or unexplained11
- Look for clues: Actively screen for subtle adaptive eating behaviors and atopic comorbidities, which may point toward EoE2,9
- Think beyond GERD: Consider EoE in younger patients or in those with GERD not controlled on proton pump inhibitors (PPIs)11
- Refer early: Send patients with dysphagia and/or suspected EoE to gastroenterology for endoscopy and biopsy to confirm diagnosis and prevent long-term complications20,21
Conclusion
Once considered rare, EoE is now recognized with increasing frequency across children and adults, making it a condition that PCPs are more likely to encounter. The key is early suspicion—dysphagia, subtle eating behavioral modifications, gastroesophageal symptoms refractory to ant-acid therapy, failure to thrive in a child with nonspecific gastrointestinal or gastroesophageal symptoms or feeding difficulties, and atopic history should raise the possibility of EoE and prompt referral to a gastroenterologist for endoscopy with biopsies. Treatment options include dietary eliminations, proton pump inhibitors, swallowed topical corticosteroids, and biologics, with the choice depending on patient preference, disease severity, and response to initial therapy. Because symptoms alone do not correlate with disease activity, routine endoscopic monitoring with histologic assessments remains essential. PCPs play a crucial role in long-term management of patients with EoE by reinforcing treatment adherence, recognizing symptom recurrence, monitoring for nutritional adequacy and treatment side effects, screening for psychosocial burden, and coordinating care across multiple specialists. By maintaining continuity and ensuring patients remain connected with specialists as needed, PCPs help optimize outcomes in this chronic disease.
Clinician and Patient Resources available at https://clinician.atpointofcare.com/eoe
