Falls are a major public health problem, occurring in more than 27% of adults 65 years and older and costing the U.S. health care system tens of billions of dollars each year. The most common risk factors are prior falls, balance disorders, fear of falling, and dementia. Regular physical activity reduces fall risk. Identifying injuries is the first step in evaluating older adults who have fallen. The patient's history may be inaccurate if they have cognitive impairment, and the physical examination can result in false-negative findings. If injury status cannot be determined and suspicion for injury remains high, clinicians can consider whole-body computed tomography (i.e., pan-scan) to evaluate the head, cervical spine, chest, abdomen, and pelvis. After addressing injuries, the next steps are to identify the cause of the fall and implement measures to reduce future fall risk. The Centers for Disease Control and Prevention has developed an easy-to-use tool to screen for and reduce fall risk, known as STEADI (Stopping Elderly Accidents, Deaths, and Injuries). An affirmative answer to any of the three STEADI screening questions indicates further evaluation with a timed up and go test, 30-second chair stand test, and four-stage balance test. If results of these tests are abnormal, multicomponent interventions are indicated to reduce future fall risk. These components include evaluating environmental and home safety factors and optimizing care of chronic medical conditions, such as diabetes mellitus, hypertension, osteoporosis, pain, urinary urgency and incontinence, and depression. Polypharmacy and drugs that increase risk of falls should be avoided, when possible. Optimization of vision and hearing correction, podiatry care, and appropriate use of ambulation devices are also important.
The World Health Organization defines falls as incidents in which a person unintentionally comes to rest on the ground or a lower level.1 They are common, occurring in more than 27% of adults 65 years and older, with 10% of those who fall reporting an injury.2 These can include head injuries, hip fracture, and other fractures such as those in the spine, pelvis, upper and lower extremities, and ribs. One-year mortality associated with hip fractures may be as high as 20% to 30%.3 Ground-level falls are the most common cause of traumatic intracranial bleeding globally, and the risk of intracranial bleeding is even higher for older adults who fall while taking combined antiplatelet therapy.4,5
WHAT'S NEW ON THIS TOPIC
| A 2023 systematic review and meta-analysis involving 70,868 community-dwelling adults found that the most common factors associated with falls in older adults are a history of falls, balance disorders, fear of falling, and dementia. |
| Although guidelines from the Centers for Disease Control and Prevention recommend treating vitamin D deficiency, one nationwide study involving more than 25,000 individuals without vitamin D deficiency found that supplementation does not decrease the risk of falls. |
| In a systematic review, multifaceted podiatric interventions (e.g., routine podiatry evaluations, provision of specialized footwear, instruction for home-based exercises, patient education) combined with multidisciplinary interventions were shown to more effectively reduce fall rates compared with a single-component intervention, such as the use of insoles. |
SORT: KEY RECOMMENDATIONS FOR PRACTICE
CDC = Centers for Disease Control and Prevention; STEADI = Stopping Elderly Accidents, Deaths, and Injuries; STOPP/START = Screening Tool of Older Persons' Prescriptions/Screening Tool to Alert to Right Treatment.
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to https://www.aafp.org/afpsort.
Falls are a serious public health issue and a major burden on the U.S. health care system. The cost of falls in older adults was estimated at $50 billion in 2015 ($64.8 billion in 2023 when adjusted for inflation).6
The risk of falls increases with age. In 2020, the Centers for Disease Control and Prevention (CDC) estimated that 14 million adults older than 65 years reported one or more falls in the previous year, and 32.9% of those individuals were older than 85 years. Older women accounted for a greater percentage of falls vs. older men (28.9% vs. 26.1%); however, men had a higher fall-related death rate when adjusted for age (91.4 per 100,000 vs. 68.3 per 100,000 in women).7
Risk Factors
A 2023 systematic review and meta-analysis involving 70,868 community-dwelling adults found that the most common factors associated with falls in older adults are a history of falls (odds ratio [OR] = 3.22; 95% CI, 1.98 to 5.23), balance disorders (OR = 3.00; 95% CI, 2.05 to 4.39), fear of falling (OR = 2.82; 95% CI, 1.68 to 4.74), and dementia (OR = 2.01; 95% CI, 1.41 to 2.86).8 Studies have also shown that older adults who report any physical activity have a lower risk of falls than those with no physical activity (24.9% vs. 33.1%; P < .001).2 Table 1 lists risk factors for falls in older adults.8–15
TABLE 1. Risk Factors for Falls in Older Adults
| Modifiable Alcohol consumption Anemia Balance disorder Chronic pain Delirium Depression Environmental risk factors Fear of falling Lack of physical activity Living alone Malnutrition Medication use (Table 3) Orthostatic hypotension Polypharmacy Sarcopenia Smoking Visual impairment | Nonmodifiable Cognitive impairment Dementia Female sex Frailty Heart disease History of falls History of stroke Hypertension Increasing age Parkinson disease Peripheral neuropathy |
Evaluation After a Fall
The initial evaluation after a fall is intended to diagnose and treat traumatic injuries and investigate the cause of the fall.16 Table 2 details a multifactorial approach to risk factor assessment after a fall.14
DIAGNOSING INJURIES
To correctly identify injuries, clinicians should perform careful full-body examinations because older patients may present atypically, and those with cognitive impairment may not be able to communicate the location of their pain. However, physical examination often does not accurately detect injuries, with false-negative rates ranging from 38% for head injuries to 80% for the cervical spine.17 Therefore, imaging is typically indicated when evaluating an older adult after a fall in an acute care setting.
Although plain radiography is usually the first imaging test, studies have shown that a negative result does not exclude fractures of the ribs, thoracic and lumbar spine, and pelvic ring. If suspicion of injuries persists after radiography, computed tomography (CT) is warranted.18 Whole-body CT (i.e., pan-scan) that includes the head, cervical spine, chest, abdomen, and pelvis can be considered.17
It is also important to determine how long the patient was on the floor. This can help identify fall-related complications from prolonged immobility such as rhabdomyolysis, dehydration, and pressure injuries.19
IDENTIFYING THE CAUSE OF THE FALL
Clinicians should investigate possible causes for the fall by obtaining a history. Specific attention should be given to mobility impairment; incorrect use of assistive devices; recent illnesses; cognitive, auditory, and visual impairment; medications, including recent medication changes; and alcohol and substance use.16 Older adults who consume alcohol are more likely to have severe head injuries after falling compared with those who avoid alcohol.20
Family members and trusted friends of the patient should be included in this conversation, if possible. They may provide details that the patient is afraid to share due to fear of loss of independence and institutionalization if they are considered unsafe to return home alone. Assessing functional status by asking about activities of daily living can help in risk assessment because lower functional status is associated with increased risk of falls.15
Elder abuse should be included in the differential diagnosis, and the patient should be assessed for inflicted injury. More information on detecting elder abuse can be found in a previous American Family Physician (AFP) review.21
ADDITIONAL EXAMINATION AND TESTING
Physical examination should include orthostatic vital signs because orthostatic hypotension is a significant risk factor for falls.13 Patients who experience transient loss of consciousness, such as syncope, also should be evaluated for cardiac arrhythmia and seizures.14 For arrhythmia, the evaluation should include 12-lead electrocardiography and consideration of an ambulatory telemetry monitor if the electrocardiography does not reveal abnormalities. If there is concern about seizures, which are more common in patients with advanced Alzheimer disease,22 electroencephalography and magnetic resonance imaging of the brain are appropriate.14
A neurologic examination should be conducted with particular focus on mental status, cranial and peripheral nerves, strength, reflexes, sensation, proprioception, and cerebellar testing to assess for neurologic causes of a fall. Neurologic causes can include stroke, Parkinson disease, dementia, peripheral neuropathy, vertigo, and peripheral nerve lesions.23,24 If the patient's history is consistent with benign paroxysmal positional vertigo, clinicians comfortable in their skillset should perform a Dix-Hallpike test and, if the result is positive, treat with an Epley maneuver.25 A video of both tests with indications is available. Other testing can include a complete metabolic panel, complete blood count, and urinalysis, which may reveal underlying conditions that led to the fall, such as anemia or infection.12 Further workup for cardiac causes can include transthoracic echocardiography.
Determining Future Fall Risk
After identifying and treating injuries and addressing any potential medical causes for the fall, the next step is to evaluate the patient's risk of future falls. Interventions can then be used to reduce the fall risk.
The CDC has developed a toolkit with resources for clinicians evaluating older adults at risk of falls. It includes the STEADI (Stopping Elderly Accidents, Deaths, and Injuries) questionnaire, which is based on joint clinical guidelines of the American Geriatrics Society and British Geriatrics Society.26
The STEADI questionnaire includes three key questions: (1) Do you feel unsteady when standing or walking? (2) Do you worry about falling? (3) Have you fallen in the past year? If the patient answers affirmatively to any of the questions, the CDC recommends further evaluation (Figure 126 ). This approach is recommended as an annual screening test or after an acute fall for community-dwelling adults older than 65 years.26
FIGURE 1.
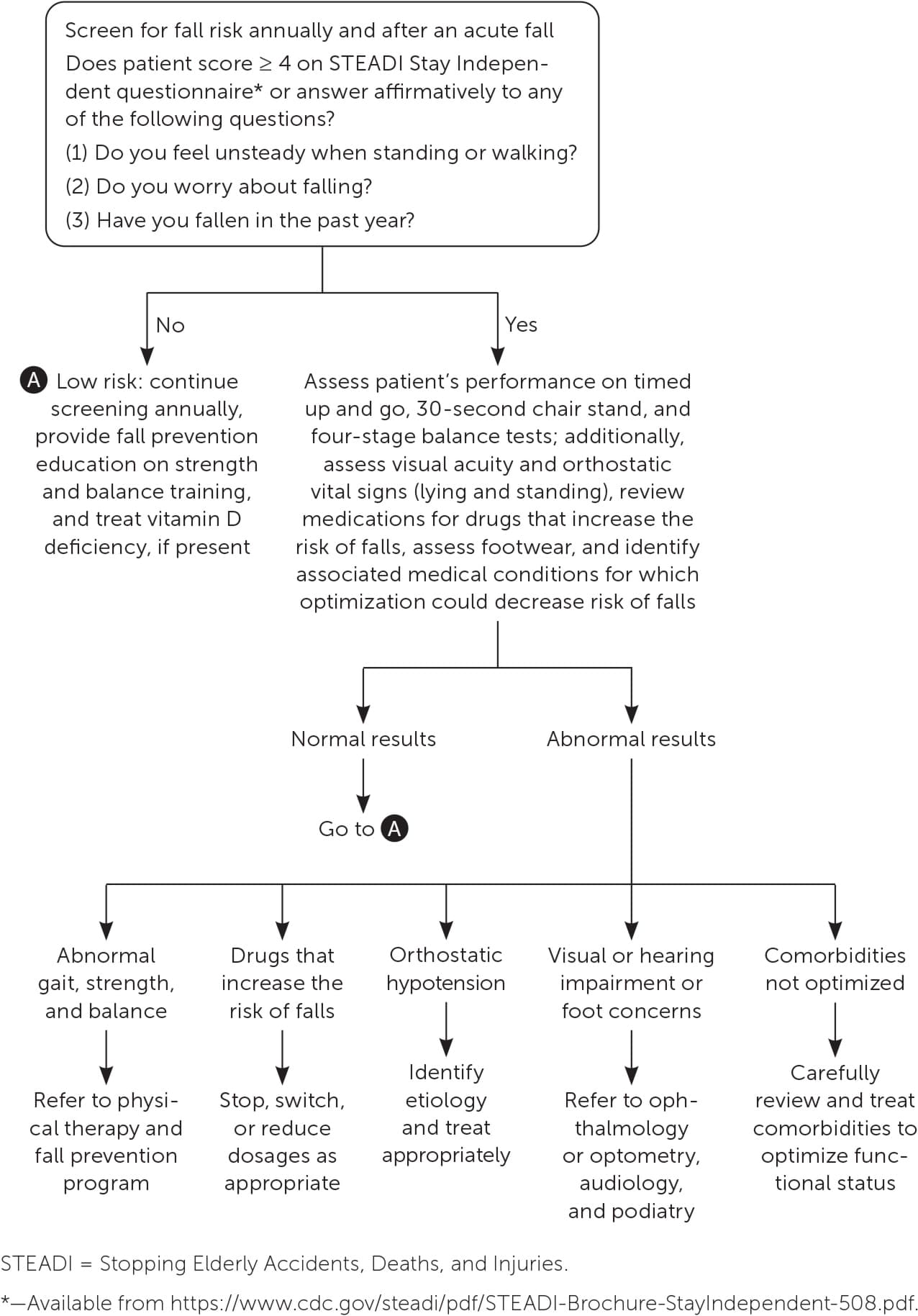
Fall risk assessment and interventions in older adults.
Adapted from Centers for Disease Control and Prevention. Algorithm for fall risk screening, assessment, and intervention. 2019. Accessed June 4, 2023. https://www.cdc.gov/steadi/pdf/STEADI-Algorithm-508.pdf.
Further evaluation should include timed up and go, 30-second chair stand, and four-stage balance tests to screen for gait, strength, and balance abnormalities.26 These tests have been used in diverse populations, including community-dwelling older adults, nursing home residents, and patients with dementia, Parkinson disease, spinal cord injuries, and cancer.27–37 They are simple to administer and relatively safe, require minimal equipment, and can help provide targeted interventional strategies for components of fall risk.27,28,38
TIMED UP AND GO TEST
For the timed up and go test, a patient stands up from a chair, walks 10 feet, turns around, then walks back to the chair and sits down.38 Older adults who complete the test in 12 or more seconds are at increased fall risk, with slower completion times indicating higher risk.
The timed up and go test has a higher specificity (0.74) than sensitivity (0.31).27 Therefore, if a result is normal, the two STEADI questions regarding previous fall history and perceived worry about falls may better predict future falls.39 A video of the timed up and go test is available.
30-SECOND CHAIR STAND TEST
The 30-second chair stand test assesses a patient's ability to stand up and sit down over 30 seconds without using their hands on the chair.29 The patient should perform as many sit-to-stand sequences as they can in the 30-second time frame while the evaluator counts complete cycles. If the patient is unable to stand without using their hands, the test result is 0. The STEADI toolkit provides age- and sex-matched normative values for the number of sit-to-stand sequences.26 A video of the 30-second chair test, including a scoring chart, is available.
FOUR-STAGE BALANCE TEST
The four-stage balance test was developed as a quick and straightforward assessment of static balance using four different foot positions. These consist of feet together, feet together with one foot a few inches forward, tandem stance (with one foot directly in front of the other), and single-leg stance. The patient should hold each position for 10 seconds. Loss of balance during any of the four stages indicates an increased risk of falls.28 A video of the four-stage balance test is available.
Evaluating Environmental Factors
In addition to various medical conditions, extrinsic and situational factors can contribute to fall risk. Extrinsic factors include elements such as inadequate lighting and obstacles on the floor. Improving lighting, highlighting or painting the edges of steps, and removing throw rugs may reduce the risk of falls at home, particularly among individuals with age-related visual impairment (e.g., cataracts, macular degeneration, glaucoma, presbyopia).40 These extrinsic factors can predispose patients to falls, especially in situations such as rushing to answer a phone call or get to the bathroom.41
It may be beneficial for clinicians to discuss these topics with the patient to mitigate fall risk. A home visit to evaluate environmental safety can also be considered; see the previous AFP article on house calls for more information.42
Optimizing Chronic Conditions
Older patients often have multiple chronic conditions, and those conditions, or the medications used to treat them, can increase the risk of falls. Several professional organizations have addressed this risk.
DIABETES MELLITUS
Older adults with diabetes and cognitive impairment are at a higher risk of falls caused by hypoglycemia, often due to incorrect administration of insulin or changes in nutritional status. As a result, current guidelines from the American Diabetes Association recommend higher glycemic targets for any older adult with a poorer health status. The American Diabetes Association also recommends screening for geriatric syndromes such as falls as a measure of function, because adults with poorer function will have higher glycemic goals.43
HYPERTENSION
Older adults taking antihypertensives who do not have other significant vascular risk factors may benefit from higher blood pressure goals. This is especially the case if they have experienced hypotensive episodes and orthostatic hypotension, defined as a decrease of 20 mm Hg in systolic blood pressure or a decrease of 10 mm Hg in diastolic blood pressure within 3 minutes after moving from a sitting to standing position.13 A 2019 systematic review and meta-analysis showed that orthostatic hypotension is positively associated with falls (OR = 1.73; 95% CI, 1.50 to 1.99).13 Continuous ambulatory blood pressure measurement is the optimal way to test for orthostatic hypotension. If it is unavailable, blood pressure can be measured at 1- and 3-minute intervals after the patient stands.13
OSTEOPOROSIS
Patients with osteoporosis diagnosed by axial dual energy x-ray absorptiometry or following a fragility fracture (i.e., low velocity fall from standing position or lower) should be treated with appropriate medications to improve bone density and reduce the risk of fall-related fractures.44
OTHER CONDITIONS
Pain and mobility impairment from arthritis or neuropathy can contribute to balance issues. Reducing pain and improving mobility may reduce fall risk.40
Urinary incontinence and lower urinary tract symptoms causing urinary urgency and the need to get to the toilet quickly can increase risk of falls. Treatment can be optimized through nonpharmacologic options such as pelvic floor therapy and timed voiding.45
Treating underlying depression through cognitive behavior therapy or pharmacotherapy can help older adults be more active and thus reduce the risk of falls. Antidepressants should be used with caution, however, because some have anticholinergic properties, which can increase fall risk.46
Although CDC guidelines recommend treating patients with vitamin D deficiency, evidence is unclear about whether vitamin D supplementation can reduce fall risk. One nationwide study involving more than 25,000 individuals without vitamin D deficiency found that supplementation does not decrease the risk of falls.47 Another study, which involved more than 600 older adults with vitamin D deficiency, found that lower dosages of vitamin D (1,000 IU per day) may reduce fall risk, but higher dosages (1,000 to 4,000 IU per day) appear to increase the risk of first-time falls and subsequent fractures.48
Optimizing Medications
Whenever possible, clinicians should avoid prescribing polypharmacy (i.e., five or more concurrent medications), drugs that increase fall risk (Table 349,50 ), and drugs that meet the American Geriatrics Society Beers Criteria for potentially inappropriate medication use in older adults.16,49,51–55
TABLE 3. Drug Classes That Increase Fall Risk
| Anticholinergics Antiemetics Antihistamines Overactive bladder and incontinence medications Skeletal muscle relaxants Antidepressants Selective serotonin reuptake inhibitors Serotonin-norepinephrine reuptake inhibitors Tricyclic antidepressants Antihypertensives/benign prostatic hyperplasia medications Agents acting on the renin-angiotensin system Alpha blockers Beta blockers Diuretics Antiparkinson drugs Adamantane derivatives Dopa and dopa derivatives Dopamine agonists Monoamine oxidase B inhibitors Other dopaminergic agents | Antipsychotics* Aripiprazole Haloperidol Olanzapine (Zyprexa) Quetiapine Risperidone Hypnotics and sedatives Benzodiazepines Alprazolam Clonazepam Diazepam Lorazepam Midazolam Nonbenzodiazepine benzodiazepine Eszopiclone (Lunesta) Zaleplon Zolpidem Opioids Codeine Hydrocodone Morphine Oxycodone Vasodilators used in cardiac disease Nitrates |
*—Does not include lithium.
A longitudinal study of 5,213 participants in England found that patients with polypharmacy had a 21% higher fall rate than those without polypharmacy. Patients taking 10 or more medications had a 50% higher rate of falls than those without polypharmacy.51
However, results of a randomized controlled trial involving 202 older adults indicate that use of certain drugs, and not just polypharmacy, increases the risk of falls. The OR for falls and in patients taking drugs that increase the risk was 2.8 (95% CI, 1.4 to 5.3; P = .001), whereas the OR for polypharmacy was only 1.6 and did not reach significance.52 This small study suggests that physicians should seek to reduce the number of prescriptions, if medically tolerated, with special attention to discontinuing drugs that increase the risk of falls.49
Not all drugs that increase the risk of falls meet the Beers Criteria, although there is significant overlap, especially with anticholinergic drugs.53 Anticholinergic burden can be measured using the Anticholinergic Burden Calculator. Medications with an anticholinergic burden score of 3, such as diphenhydramine, increase the risk of falls by more than 50% compared with medications with no anticholinergic effect.54
Community-dwelling older adults at low risk of falls should be assessed yearly. If they experience a fall, they should receive education on fall prevention and participate in an exercise program.16 Clinicians should also review medications at each visit to determine whether they can deprescribe any medications, either by decreasing the dosage of a medication or stopping a medication when the patient's health status changes or the benefits no longer outweigh the risks. Validated tools such as STOPP/START (Screening Tool of Older Persons' Prescriptions/Screening Tool to Alert to Right Treatment) can guide clinicians in deprescribing.56
Other Interventions
MULTICOMPONENT PROGRAMS
For patients at higher risk of falls, more comprehensive multicomponent interventions are appropriate. A 2018 Cochrane review found that compared with standard care, multicomponent interventions are more effective at reducing the risk of falls.57 These interventions include components such as the Otago Exercise Program, progressive resistance or high-intensity strength training with weights or machines, gait training such as walking outdoors or climbing stairs, and tai chi.58,59 Patients are most likely to recall and adhere to exercise prescriptions provided by a physical therapist.60
Other multicomponent interventions shown to reduce fall risk include occupational therapy fall reduction programs, appropriate prescription of assistive devices, fall prevention education (e.g., strength and balance training), and caregiver education when delivered by occupational therapist.61
HOME MODIFICATIONS
Home modifications to reduce falls include improving lighting, removing trip hazards (e.g., throw rugs, pets, oxygen tubing), avoiding inappropriate footwear, addressing unsafe stairways and irregular floors, and modifying bedrooms and bathrooms based on the patient's mobility level.62
VISION MANAGEMENT
Optometrists can reduce fall risk by addressing visual acuity, titrating prescriptions to allow eyes to adjust with each new prescription, and recommending against multifocal lenses (e.g., bifocal and progressive lenses).63 These lenses have been implicated in increasing fall risk in older adults due to impaired depth perception and edge contrast sensitivity (i.e., the ability to distinguish the edges of objects in low light). Ophthalmologists play a key role in treating macular degeneration, cataracts, and glaucoma because patients with these diseases have an increased risk of falls and fractures.64
HEARING TREATMENT
The prevalence of hearing loss in adults older than 60 is between 33% and 40%. Patients with hearing loss experience a dose-response relationship in which those with the most severe hearing loss are at the highest risk of falling. Referral to audiology is an important component of managing fall risk in this population.65
PODIATRIC INTERVENTIONS
In a systematic review, multifaceted podiatric interventions (e.g., routine podiatry evaluations, provision of specialized footwear, instruction for home-based exercises, patient education) combined with multidisciplinary interventions were shown to more effectively reduce fall rates when compared with single-component interventions, such as the use of insoles. A referral to podiatry would thus be appropriate to help reduce fall risk as part of routine intervention.66
ASSISTIVE DEVICES
Assistive devices can help prevent falls by improving safety and confidence with mobility and providing patients with more independence to complete activities of daily living. However, using the wrong assistive device or using it improperly is unsafe.67 Assistive device assessment and training should be part of fall prevention interventions. Clinicians should be trained to select suitable mobility devices or consult a physical therapist. A previous AFP article on mobility assistive devices also provides guidance.67
APP-BASED INTERVENTIONS
There are many app-based technologies that are feasible for use by older adults with fall risk. One example is the Nymbl Training app. It uses an evidence-based approach derived from the STEADI toolkit to implement balance training for older adults. In a feasibility study, participants reported that this app was beneficial, easy to incorporate into their routine, and appropriate for balance training.68 Another example is Keep On Keep Up, a strength and balance training app designed specifically for low-income older adults who have difficulty engaging in community resources due to immobility.69 Research is ongoing to further examine the effectiveness of these and other technology-based approaches to fall prevention.
Data Sources: A PubMed search was completed in Clinical Queries using the key terms falls and elderly. The search included meta-analyses, randomized controlled trials, clinical trials, and reviews. The Agency for Healthcare Research and Quality Effective Healthcare Reports, the Cochrane database, DynaMed, and Essential Evidence Plus were also searched. Search dates: May 5, 2023, and March 8, 2024.
The opinions and assertions contained herein are the private views of the authors and are not to be construed as official or as reflecting the views of the U.S. Army, the U.S. Department of Defense, or the U.S. government.
The authors give special thanks to Carrie Rubenstein, MD, program director of the Geriatric Medicine Fellowship at Swedish Medical Center, for guidance.
