Acute pericarditis is defined as inflammation of the pericardium and occurs in approximately 4.4% of patients who present to the emergency department for nonischemic chest pain, with a higher prevalence in men. Although there are numerous etiologies of pericarditis, most episodes are idiopathic and the cause is presumed to be viral. Diagnosis of pericarditis requires at least two of the following criteria: new or worsening pericardial effusion, characteristic pleuritic chest pain, pericardial friction rub, or electrocardiographic changes, including new, widespread ST elevations or PR depressions. Pericardial friction rubs are highly specific but transient, and they have been reported in 18% to 84% of patients with acute pericarditis. Classic electrocardiographic findings include PR-segment depressions; diffuse, concave, upward ST-segment elevations without reciprocal changes; and T-wave inversions. Transthoracic echocardiography should be performed in all patients with acute pericarditis to characterize the size of effusions and evaluate for complications. Nonsteroidal anti-inflammatory drugs are the first-line treatment option. Glucocorticoids should be reserved for patients with contraindications to first-line therapy and those who are pregnant beyond 20 weeks' gestation or have other systemic inflammatory conditions. Colchicine should be used in combination with first- or second-line treatments to reduce the risk of recurrence. Patients with a higher risk of complications should be admitted to the hospital for further workup and treatment.
Acute pericarditis, or inflammation of the pericardium, has numerous etiologies and often produces a characteristic pleuritic chest pain. This article reviews patient-oriented evidence to guide the diagnosis and management of acute pericarditis.
SORT: KEY RECOMMENDATIONS FOR PRACTICE
| Clinical recommendation | Evidence rating | Comments |
|---|---|---|
| Evaluation of acute pericarditis should include a patient history, physical examination, electrocardiography, chest radiography, transthoracic echocardiography, and baseline laboratory studies.6 | C | Expert consensus guidelines |
| All patients with acute pericarditis should be treated with colchicine (Colcrys) and nonsteroidal anti-inflammatory drugs or glucocorticoids to reduce the risk of recurrence.35–38 | A | Systematic reviews and meta-analyses with patient-oriented outcomes |
| Patients with acute pericarditis who have risk factors for serious disease or complications should be hospitalized for further treatment and etiologic workup.6,20 | B | Two prospective cohort studies |
| Athletes with acute pericarditis should not participate in competitive sports for 3 months after being diagnosed or for 3 to 6 months in those with myopericarditis.6,45 | C | Expert consensus guidelines |
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to https://www.aafp.org/afpsort.
Epidemiology
- In one small study, acute pericarditis was diagnosed in 4.4% of patients admitted to the emergency department with nonischemic chest pain; it accounts for 0.2% of cardiovascular hospital admissions.1,2 The exact incidence of acute pericarditis is difficult to estimate because epidemiologic studies are lacking, and mild cases likely resolve without being formally diagnosed.3,4
- Acute pericarditis occurs mostly in adult patients, with a mean age in the 50s.3–9 Hospital registry data suggest that men are more likely to be affected by acute pericarditis than women, with incidence ratios of 1.7 to 2.0 in men to 1.0 in women.2–5
- Acute pericarditis is typically a result of systemic disease or related to processes involving the pericardium3,6,9–15 (eTable A).
- Despite advances in diagnostic testing, more than 50% of episodes are idiopathic and the etiology is presumed to be viral.3,5 Pericarditis after cardiac injury is emerging as the second leading cause of pericarditis and occurs in 9% to 33% of patients.3,5,6,9–14
- Tuberculosis accounts for up to 70% of pericarditis in endemic areas but is a rare etiology in nonendemic areas.9–14,16
eTABLE A Etiologies of Acute Pericarditis
| Acute/idiopathic Drug related Antineoplastic drugs (e.g., cyclophosphamide, cytarabine, daunorubicin, doxorubicin, fluorouracil) Bromocriptine (Parlodel) Clozapine Cyclosporine Dantrolene (Dantrium) Granulocyte-macrophage colony-stimulating factor Lupus-like syndrome (e.g., hydralazine, isoniazid, methyldopa, phenytoin, procainamide) Mesalamine Methysergide Minoxidil para-aminosalicylic acid Penicillins Practolol Some vaccines Streptomycin Sulfa drugs Thiazides Thiouracils Tumor necrosis factor inhibitors Metabolic Anorexia nervosa Myxedema Uremia Other Dissecting aortic aneurysm Heart failure Pulmonary arterial hypertension | Infectious Bacterial Actinomyces neuii Borrelia burgdorferi Chlamydia spp. Coxiella burnetii Haemophilus spp. Klebsiella pneumoniae Legionella spp. Leptospira spp. Listeria spp. Mycobacterium tuberculosis Mycoplasma spp. Neisseria meningitidis Photobacterium damselae Providencia stuartii Pseudomonas aeruginosa Salmonella spp. Staphylococcus spp. Streptococcus spp. Syphilis spp. Tropheryma whipplei Fungal Aspergillus spp. Blastomyces spp. Candida spp. Coccidioides spp. Cryptococcus spp. Histoplasma spp. | Viral Adenoviruses Enteroviruses (e.g., coxsackievirus, echovirus) Hepatitis A, B, and C Herpesviruses (e.g., cytomegalovirus, Epstein-Barr virus, human herpesvirus type 6, varicella-zoster virus) HIV Influenza Parainfluenza Parvovirus B19 Other Echinococcus spp. Löffler syndrome Toxoplasma spp. Noninfectious Autoimmune/inflammatory Ankylosing spondylitis Dermatomyositis Familial Mediterranean fever Inflammatory bowel diseases Lupus erythematosus Rheumatoid arthritis Sarcoidosis Scleroderma Sjögren syndrome Still disease Systemic vasculitides (e.g., Behçet syndrome, eosinophilic granulomatosis with polyangiitis, giant cell arteritis, Takayasu arteritis) | Neoplasms Primary tumors (e.g., fibroma, lipoma, mesothelioma, pericardial cardiac angiosarcoma) Secondary tumors (e.g., adenocarcinoma of the breast, colon, cystic duct, kidney, liver, and lung; bladder carcinoma; cholangiocarcinoma; gastric carcinoma; leukemia; lymphoma; mediastinal sarcoma; melanoma; mesothelioma; myeloma; ovarian tumor; papillary thyroid carcinoma; renal cell carcinoma; small cell lung carcinoma; squamous cell uterine carcinoma) Traumatic and iatrogenic Esophageal perforation Pancreatitis Penetrating and nonpenetrating thoracic injury Pericardial injury syndromes (e.g., postmyocardial infarction syndrome, postpericardiotomy syndrome, posttraumatic/procedural [after bypass surgeries, coronary percutaneous intervention, left atrial appendage exclusion, pacemaker lead insertion, radiofrequency ablation, and valve repair or replacement]) Radiation injury |
Information from:
Adler Y, Charron P, Imazio M, et al.; ESC Scientific Document Group. 2015 ESC guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Disease s of the European Society of Cardiology (ESC) endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2015;36(42):2921–2964.
Ariyarajah V, Spodick DH. Acute pericarditis: diagnostic cues and common electrocardiographic manifestations. Cardiol Rev. 2007;15(1):24–30.
Fallek Boldes O, Dahan S, Segal Y, et al. Characteristics of pericardial biopsy: 100 cases in a single center. Isr Med Assoc J. 2019;21(3):183–188.
Gouriet F, Levy PY, Casalta JP, et al. Etiology of pericarditis in a prospective cohort of 1162 cases. Am J Med. 2015;128(7):784.e1–784.e8.
Levy PY, Fournier PE, Charrel R, et al. Molecular analysis of pericardial fluid: a 7-year experience. Eur Heart J. 2006;27(16):1942–1946.
Sathirareuangchai S, Kobayashi M, Shimizu D. Etiologies of pericarditis in hospital and forensic autopsies. Cardiovasc Pathol. 2020;49:107262.
Shakti D, Hehn R, Gauvreau K, et al. Idiopathic pericarditis and pericardial effusion in children: contemporary epidemiology and management. J Am Heart Assoc. 2014;3(6):e001483.
Snyder MJ, Bepko J, White M. Acute pericarditis: diagnosis and management. Am Fam Physician. 2014;89(7):553–560.
Zayas R, Anguita M, Torres F, et al. Incidence of specific etiology and role of methods for specific etiologic diagnosis of primary acute pericarditis. Am J Cardiol. 1995;75(5):378–382.
Diagnosis
- Diagnosis of pericarditis requires at least two of the following criteria: new or worsening pericardial effusion, characteristic pleuritic chest pain, pericardial friction rub, or electrocardiographic (ECG) changes, including new, widespread ST elevations or PR depressions.6,17
- Pericarditis can be further classified as acute, incessant, recurrent, or chronic.6
- The differential diagnosis includes other causes of acute chest pain, such as thoracic artery aneurysm and dissection, acute coronary syndrome, mediastinitis, pulmonary embolism, pneumonia, pneumothorax, pneumopericardium, costochondritis, gastroesophageal reflux disease, neoplasm, or myocarditis (Table 1).6,10,18,19
TABLE 1. Differential Diagnosis of Acute Pericarditis and Associated Electrocardiographic Findings
| Diagnosis | Symptoms/signs | Electrocardiographic findings | Biomarkers |
|---|---|---|---|
| Acute pericarditis | Retrosternal, sharp, pleuritic chest pain exacerbated by a supine position and relieved by leaning forward; radiation to jaw, arm, or neck; friction rub | PR-segment depression; diffuse, concave ST-segment elevations without reciprocal depressions; T-wave inversion | Troponin elevated in 30% of cases; normal BNP |
| Myocardial infarction | Crushing, squeezing, retrosternal chest pain; dyspnea; radiation to jaw, arm, or neck | ST-segment elevation, ST-segment depression, T-wave inversion | Troponin elevated; mild elevation of BNP |
| Myocarditis | Chest pain; dyspnea; signs of heart failure may be present | Nonspecific ST-segment and T-wave changes | Troponin elevated; mild elevation of BNP |
| Pulmonary embolism | Sharp, stabbing chest pain that may be anterior, posterior, or lateral; may be worse with respiration | Right axis deviation; signs of right ventricular strain (ST-segment depression, T-wave inversion in right precordial leads V1 to V3) | Troponin and BNP may be elevated in submassive or massive pulmonary embolism; used prognostically |
BNP = brain natriuretic peptide.
SIGNS AND SYMPTOMS
- More than 90% of patients being evaluated for acute pericarditis report acute, retrosternal, pleuritic chest pain. Pain may radiate to the jaw, neck, or arms, but this should not be considered sensitive or specific for acute pericarditis.6,20,21
- Pain may be exacerbated by a supine position or improved by leaning forward.6 In one cohort study, 46% of patients with pericarditis diagnosed in the emergency department experienced changes in pain with changes in posture.21
- Pain is not generally relieved by nitrates.6,10,17
- Patients with an infectious etiology of acute pericarditis may have fever, chills, myalgias, tachycardia, and leukocytosis.6,22
- Pericardial friction rubs are highly specific for pericarditis but have low sensitivity, with 18% to 84% of patients having a pericardial friction rub.7,23,24 Friction rub is characterized by a transient, scratchy or squeaky quality that is best auscultated by the patient leaning forward and holding their breath.6,10,17,21 An audible example of a friction rub is available.
- Acute pericarditis can be complicated by cardiac tamponade, which is suggested by hypotension, pulsus paradoxus, increased jugular venous pressure, and a quiet precordium.6
DIAGNOSTIC TESTING
Initial Evaluation
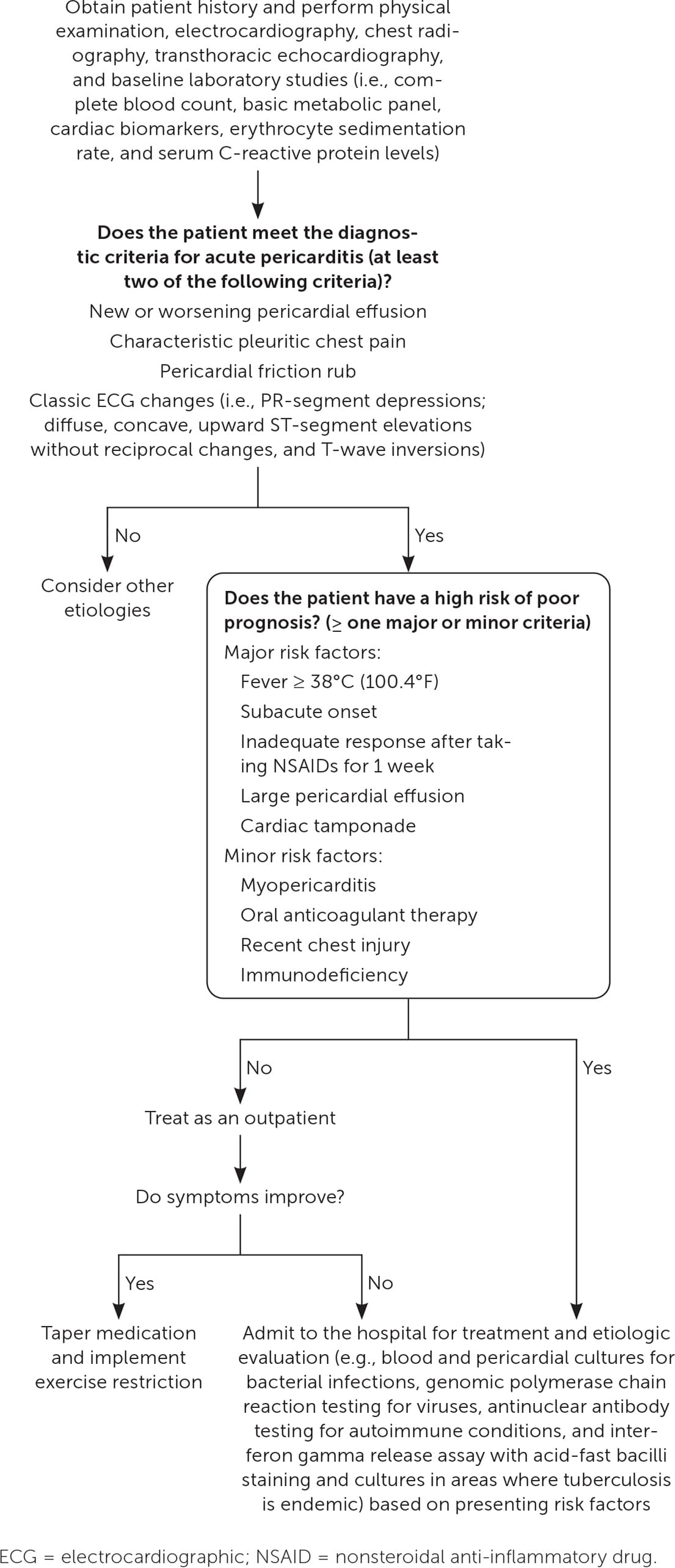
- The initial evaluation should include patient history, physical examination, electrocardiography, chest radiography, transthoracic echocardiography, and baseline laboratory studies (i.e., complete blood count, basic metabolic panel, cardiac biomarkers, erythrocyte sedimentation rate, and serum C-reactive protein levels).6
- Classic ECG f indings include PR-segment depressions; diffuse, concave, upward ST-segment elevations without reciprocal changes; and T-wave inversions (Figure 110 ). These findings are common but are not present in all cases.6,21
- In contrast, ECG findings suggestive of ischemia or infarction include convex ST elevations that are regional without reciprocal ST depressions. PR depression is generally absent.25,26
- Elevation of C-reactive protein levels occurs in approximately 75% of patients suspected of having acute pericarditis; although it is not diagnostic, elevation can support the diagnosis.27
- In a retrospective observational study, an elevated neutrophil-lymphocyte ratio of 5.0 or greater was associated with an increased probability of recurrence of pericarditis and cardiac tamponade (odds ratio = 2.4; 95% CI, 1.7 to 3.4).28
- Cardiac biomarkers were elevated in 6.4% to 49% of patients in three observational studies.21,29,30 In one cohort study, an increase in serum troponin levels was associated with one additional day of hospitalization.31
- Chest radiography can detect an enlarged cardiac silhouette, which supports the presence of pericardial effusion.6
- Transthoracic echocardiography is recommended for evaluation of patients with acute pericarditis because it can identify potential complications, such as tamponade or constrictive pericarditis.10,18
- Transthoracic echocardiography can indirectly quantify the size of pericardial effusion. Pericardial effusions larger than 21 mm on echocardiography are associated with a higher risk of complications.18
- In patients with suspected viral pericarditis, routine identification of the causative agent is not recommended unless hepatitis C or HIV infection is suspected.17
FIGURE 1.
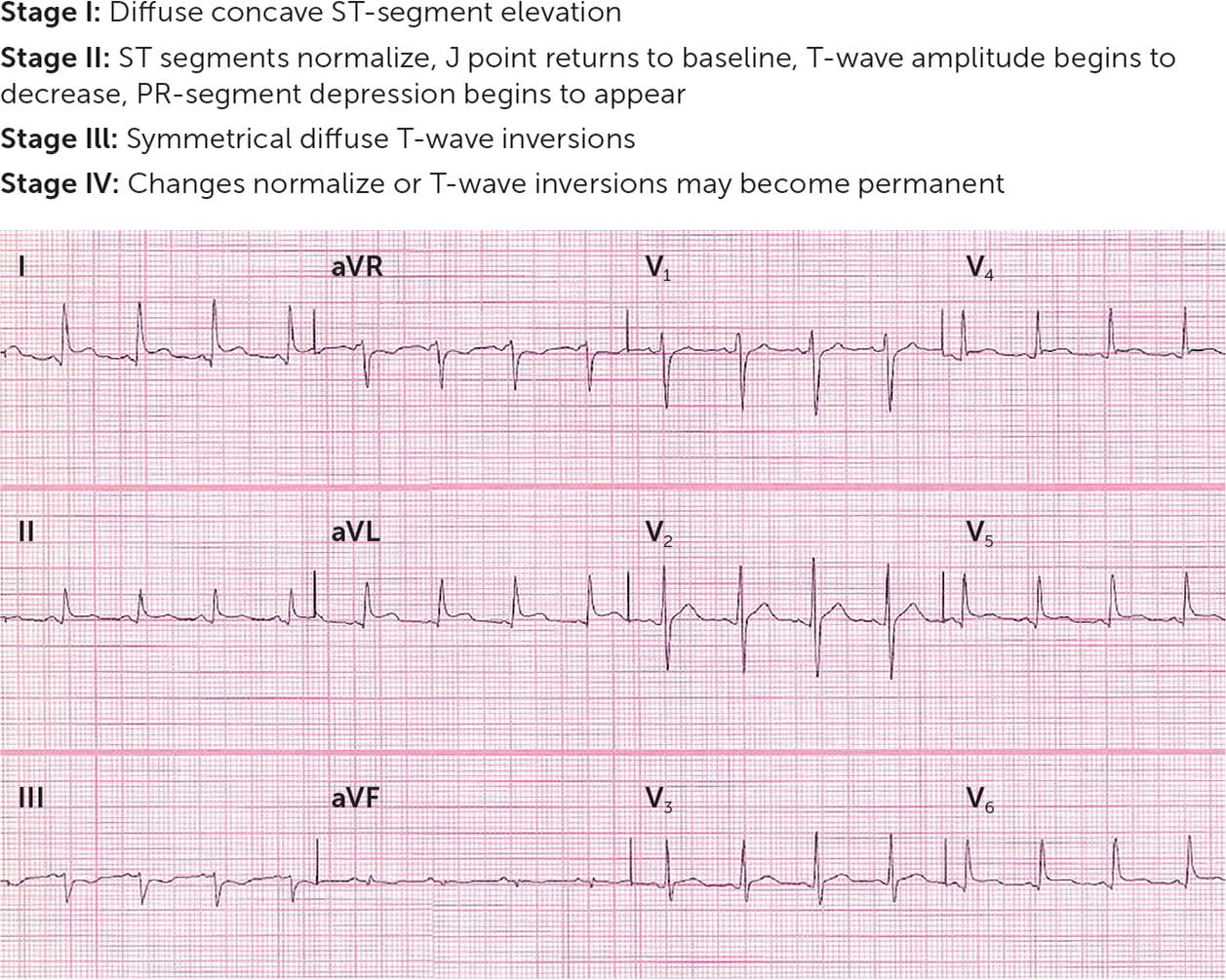
Acute pericarditis electrocardiographic changes, stage I. Diffuse, concave ST-segment elevation and PR-segment depression are best demonstrated in leads I, II, aVL, and V3 to V5. Also note ST/T ratio > 0.25 in V6 (vertical height of ST segment from end of PR segment to J point/amplitude of T wave) and lack of reciprocal ST-segment changes.
Adapted with permission from Snyder MJ, Bepko J, White M. Acute pericarditis: diagnosis and management. Am Fam Physician. 2014;89(7):557.
Subsequent Testing for High-Risk or Hospitalized Patients
- For patients who require hospitalization, evaluation should include obtaining blood and pericardial cultures to identify bacterial infections, genomic polymerase chain reaction testing to identify viruses, and antinuclear antibody testing to identify autoimmune conditions.6,20
- Computed tomography and cardiac magnetic resonance imaging are considered adjunct studies that could identify pericardial effusion or evidence of myocardial inflammation.18 In a retrospective observational study, pericardial thickening or enhancement was the most accurate single parameter for pericarditis, with a sensitivity of 54% to 59% and a specificity of 91% to 96% (positive likelihood ratio = 8.1; negative likelihood ratio = 0.46).32
- Tuberculosis testing using interferon gamma release assay with acid-fast bacilli staining and cultures should be considered in areas where tuberculosis is endemic.17,33
Treatment
- First-line treatment includes nonsteroidal anti-inflammatory drugs (NSAIDs), colchicine (Colcrys), and a proton pump inhibitor for gastro-protection. Ibuprofen and indomethacin are the most commonly used NSAIDs; aspirin is preferred in patients with comorbid coronary artery disease.6,34
- Expert opinion suggests that NSAIDs should be used for 7 to 10 days followed by a gradual taper once symptoms improve and C-reactive protein levels normalize.27
- Glucocorticoids are typically second-line therapy or used when NSAIDs are contraindicated (e.g., beyond 20 weeks' gestation, systemic inflammatory disease) due to a higher risk of recurrence and adverse effects. Prednisone dosages of 0.25 to 0.5 mg per kg per day followed by a slow taper minimize the risk of recurrence compared with higher dosages.6
- The addition of colchicine to first- or second-line agents significantly reduces the recurrence rate of acute pericarditis (absolute risk reduction = 22%; number needed to treat = 5) and recurrent pericarditis (absolute risk reduction = 23%; number needed to treat = 4). Colchicine should be used for 3 months in patients with acute pericarditis and at least 6 months in those with recurrent pericarditis.35–38
- Triple therapy with NSAIDs, glucocorticoids, and colchicine may be used in patients with recurrent pericarditis refractory to standard care, based on expert opinion and an observational study. If symptoms recur during glucocorticoid tapering, it is preferred to restart by increasing the dosage of the NSAID, not increasing the dosage of the glucocorticoid.6,39,40
- Use of anti–interleukin-1 agents, such as anakinra and rilonacept (Arcalyst), for the treatment of recurrent pericarditis refractory to standard treatment is supported by two small randomized controlled trials. A retrospective cohort study and a systematic review show weaker evidence for the use of azathioprine and intravenous immune globulin, respectively.6,41–44
- Pericardiocentesis may be performed for cardiac tamponade, for suspected bacterial or neoplastic etiology, or for symptomatic effusions that have not responded to standard therapy.6
- Major risk factors derived from multivariate analysis and minor risk factors derived from expert opinion are associated with a worse prognosis and should prompt consideration for hospital admission and further workup (Figure 2).6,20
- Based on expert opinion, athletes should not participate in competitive sports for 3 months after the diagnosis of acute pericarditis and 3 to 6 months if there is myopericarditis. It is reasonable to return to play in less time if serum biomarkers, left ventricular function, and ECG findings have normalized.6,45
Prognosis
- Mortality in acute pericarditis is low, with a rate of 1.1% in hospitalized patients.2
- Idiopathic pericarditis is generally self-limited and responds well to initial treatment within a few days. Less than 5% of patients experience poor symptom resolution with initial treatment.6,35,37
- Symptoms recur in 10% to 30% of patients despite an initial satisfactory response to treatment with an NSAID and colchicine.35,37,46
- Significant complications can include pericardial effusion causing cardiac tamponade, left ventricular dysfunction, arrhythmias, heart failure, and constrictive pericarditis.6,47
- Although patients with idiopathic recurrent pericarditis experience higher morbidity, serious late complications, including tamponade, left ventricular dysfunction, and constrictive pericarditis, are rare.40,47,48
This article updates previous articles on this topic by Snyder, et al.10; Tingle, et al.49; Goyle and Walling50; and Marinella.51
Data Sources: A PubMed search was completed in Clinical Queries using the key term pericarditis. The search included meta-analyses, randomized controlled trials, clinical trials, and reviews. Essential Evidence Plus, POEMs, the Cochrane database, DynaMed, and UpToDate were also searched. Whenever possible, if studies used race and/or gender as patient categories but did not define how these categories were assigned, they were not included in our final review. If studies using these categories were determined to be essential and were therefore included, limitations were explicitly stated in the manuscript. Search dates: April, June, and November 2023, and March 2024.
The views expressed are those of the authors and do not reflect the official policy of the Madigan Army Medical Center, Uniformed Services University of the Health Sciences, U.S. Department of the Army, U.S. Department of Defense, or U.S. government.
