Carpal tunnel syndrome (CTS) is caused by compression of the median nerve as it travels through the carpal tunnel. Patients commonly experience pain, paresthesia, and, less often, weakness in the distribution of the median nerve. Provocative maneuvers, such as the Phalen test and Tinel sign, have varying sensitivity and specificity for the diagnosis of CTS. Thenar atrophy is a late finding and highly specific for CTS. Although patients with a classic presentation of CTS do not need additional testing for diagnosis, electrodiagnostic studies can confirm the diagnosis in atypical cases, exclude other causes, and gauge severity for surgical prognosis. An abnormal nerve conduction study is useful for ruling in CTS, but a normal test does not necessarily exclude it. Over-the-counter analgesics, such as nonsteroidal anti-inflammatory drugs and acetaminophen, have not shown benefit for CTS. Patients with mild to moderate CTS initially may be offered nonsurgical treatments, such as splinting or local corticosteroid injections. Night-only splinting is as effective as continuous wear. A neutral wrist splint may be more effective than an extension splint. In patients with recent onset of CTS, corticosteroid injections provide slightly greater improvement of symptoms compared with splinting at 6 weeks, with similar outcomes at 6 months. Patients with severe CTS, including objective weakness or sensory deficits, should be offered surgical decompression. Endoscopic and open carpal tunnel release techniques are equally effective.
Carpal tunnel syndrome (CTS), caused by compression of the median nerve as it travels through the carpal tunnel, is the most common entrapment neuropathy of the upper extremity. This article provides a brief summary of the best available patient-oriented evidence for CTS.
SORT: KEY RECOMMENDATIONS FOR PRACTICE
| Clinical recommendation | Evidence rating | Comments |
|---|---|---|
| Splinting may be effective for relief of mild to moderate carpal tunnel symptoms. Neutral splints are more effective than extension splints, and night-only wear is as effective as continuous wear.15–17 | B | Limited evidence from meta-analysis of multiple RCTs |
| Local corticosteroid injections improve symptoms and function in patients with carpal tunnel syndrome for up to 6 months and decrease the need for surgery at 1 year.19 | A | Consistent, patient-oriented evidence from meta-analysis of RCTs |
| Endoscopic and open carpal tunnel release techniques are equally effective, with high long-term response rates and minimal complications.28–30 | A | Consistent evidence from RCTs with long-term follow-up |
| Postoperative splinting and rehabilitation are not effective.31 | B | Lack of benefit and inconsistent evidence from meta-analysis of multiple low-quality RCTs |
RCT = randomized controlled trial.
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to https://www.aafp.org/afpsort.
EPIDEMIOLOGY
- The incidence of CTS in the United States is estimated to be 3.8 per 1,000 person-years and increases with age.1 Risk factors include a body mass index greater than 25 kg per m2, activities with repetitive or forceful wrist motion, female sex, diabetes mellitus, arthritis, pregnancy, and hypothyroidism.2–4
DIAGNOSIS
Signs and Symptoms
- CTS is clinically diagnosed in a patient with typical symptoms and physical examination findings (Table 1). A video demonstrating common physical examination tests for CTS is available.
- Patients typically present with pain and paresthesia in the median nerve distribution—the first three digits of the hand and the radial half of the fourth—that often disturb sleep and improve with hand position changes. Weakness of thumb opposition or abduction that cause hand clumsiness may occur in severe cases. Symptoms can vary widely and may include the entire hand and pain radiating proximally (Figure 15).
- The upper extremities and neck should be evaluated to exclude causes such as cervical radiculopathy (Table 26).
- Thenar atrophy, which occurs in severe cases, has a specificity of up to 99% for CTS.4
- Provocative maneuvers, such as the Phalen test and Tinel sign, can help clinically diagnose CTS. However, individually, these tests have poor sensitivity and specificity. A recent meta-analysis of more than 20 studies found a pooled sensitivity of 57% (95% CI, 44% to 68%) and specificity of 67% (95% CI, 52% to 79%) for the Phalen test and a pooled sensitivity of 45% (95% CI, 34% to 57%) and specificity of 67% (95% CI, 60% to 89%) for the Tinel sign.7
- A combination of findings is more predictive than a single maneuver. The CTS-6 is a clinical prediction rule that includes six clinical findings. A score of 12 or greater has an 80% probability for CTS (Table 3).8
TABLE 1. Common Physical Examination Maneuvers for Carpal Tunnel Syndrome
| Maneuver | Description |
|---|---|
| Closed fist sign* | Patient makes a fist and holds for 60 seconds |
| Hand elevation test* | Patient raises hands above their head for 60 seconds |
| Loss of two-point discrimination | Inability to discriminate between two points held ≤ 5 mm apart from one another on the palmar side of the first, second, or third digits |
| Manual carpal compression test* | Apply direct pressure on the volar wrist surface over the carpal tunnel for 30 seconds |
| Phalen test* | Flex patient's wrist 90 degrees with elbow in full extension for 60 seconds |
| Tinel sign* | Rapidly percuss the volar surface of the wrist proximal to the wrist crease/over the carpal tunnel. |
*—These maneuvers are considered positive if pain or paresthesia occur in the median nerve distribution while performing the test.
Common Physical Examination Tests for Carpal Tunnel Syndrome
FIGURE 1.
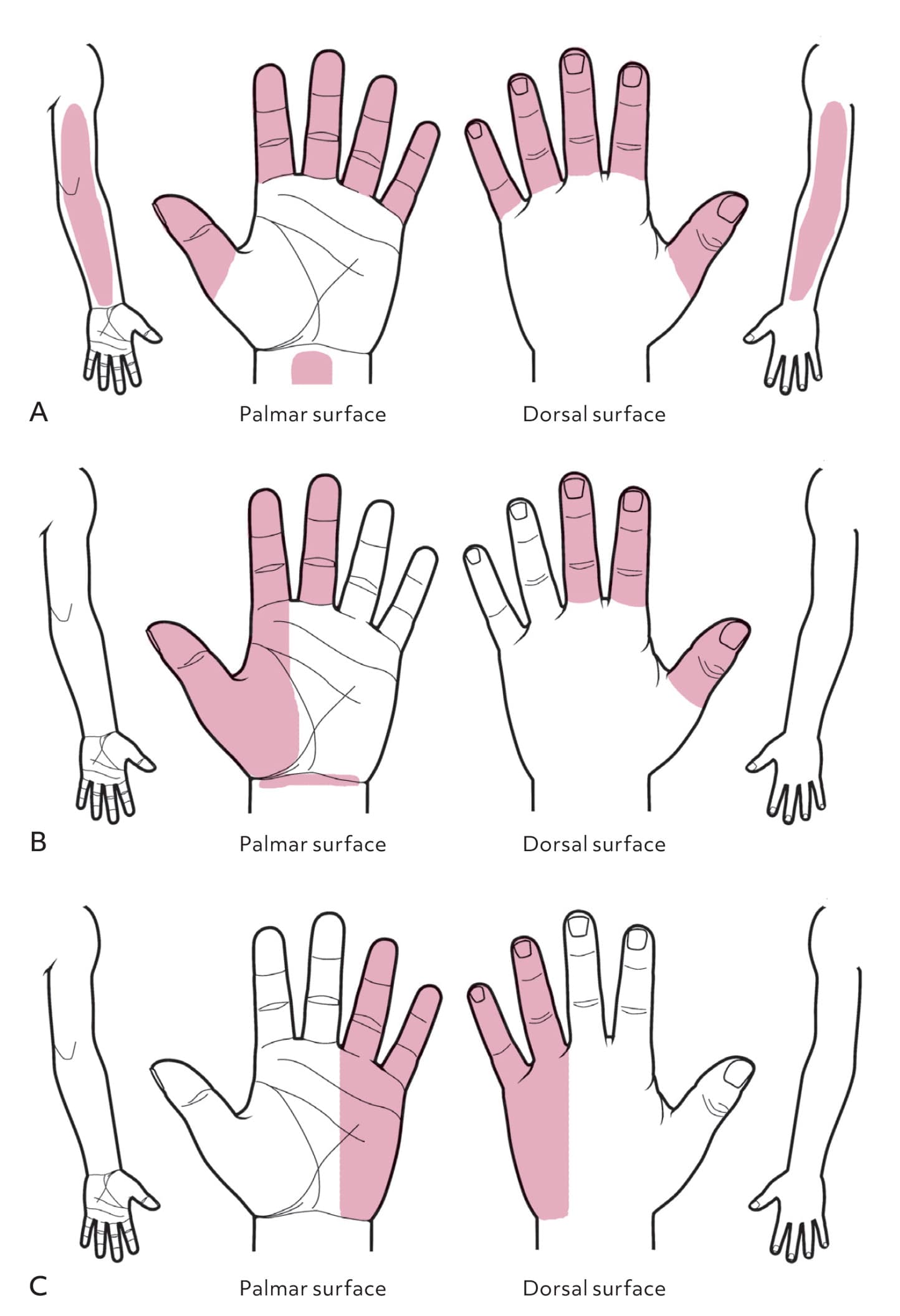
Katz hand diagram. A hand symptom diagram can be a useful tool in diagnosing carpal tunnel syndrome. (A) In the classic pattern, symptoms affect at least two of digits 1, 2, or 3. It includes symptoms in the fourth and fifth digits, wrist pain, and radiation of pain proximal to the wrist but excludes symptoms on the palm or dorsum of the hand. (B) The probable pattern has the same symptom pattern as the classic pattern, except palmar symptoms are possible unless confined solely to the ulnar aspect. In the possible pattern (not shown), symptoms involve only one of digits 1, 2, or 3. (C) In the unlikely pattern, no symptoms are present in digits 1, 2, or 3.
Redrawn by Dave Klemm
Adapted with permission from Katz JN, Stirrat CR, Larson MG, et al. A self-administered hand symptom diagram for the diagnosis and epidemiologic study of carpal tunnel syndrome. J Rheumatol. 1990;17(11):1497.
TABLE 3. CTS-6: A Clinical Aid for Diagnosing Carpal Tunnel Syndrome
| Symptoms and history | |
| Numbness predominantly or exclusively in median nerve territory Sensory symptoms are mostly in the thumb, index, middle and/or ring fingers | 3.5 |
| Nocturnal numbness Symptoms are prominent when patient sleeps; numbness wakes patient from sleep | 4 |
| Physical examination | |
| Thenar atrophy and/or weakness The bulk of the thenar area is reduced or manual motor testing shows strength of grade 4 or less | 5 |
| Positive Phalen test Flexion of the wrist reproduces or worsens symptoms of numbness in the median nerve territory | 5 |
| Loss of 2-point discrimination A failure to discriminate two points held 5 mm or less apart from one another, in the median nerve innervated digits, is a positive test suggestive of CTS | 4.5 |
| Positive Tinel sign Light tapping over the median nerve at the level of the carpal tunnel causing radiating paraesthesiae into the median nerve innervated digits (not proximally) is a positive test | 4 |
Note: The corresponding point values for all positive findings are added together to obtain a total score. A score of 12 or greater is defined as positive for carpal tunnel syndrome.
CTS = carpal tunnel syndrome.
Reprinted with permission from Graham B. The value added by electrodiagnostic testing in the diagnosis of carpal tunnel syndrome. Bone Joint Surg Am. 2008;90(12):2590.
Diagnostic Testing
- Electrodiagnostic studies help confirm the diagnosis in atypical presentations, exclude other causes, and determine severity for surgical prognosis. However, studies report varying diagnostic accuracy.
- Nerve conduction studies are used to confirm CTS, but results are normal in up to 15% to 25% of patients.9 The sensitivity and specificity of nerve conduction studies vary from 56% to 85% and 94% to 99%, respectively.10,11 Therefore, a positive test result is useful for ruling in CTS, but a negative result does not exclude CTS, especially in mild cases.
- Electromyography assesses pathologic changes in muscles innervated by the median nerve, which helps gauge severity and exclude other causes.
- Axon loss or muscle denervation signifies severe disease and should prompt referral for surgery.4
- Ultrasonography of the cross-sectional area of the median nerve has been evaluated for the diagnosis of CTS; however, evidence is limited due to varying protocols and lack of consensus regarding the optimal diagnostic threshold.12
TREATMENT
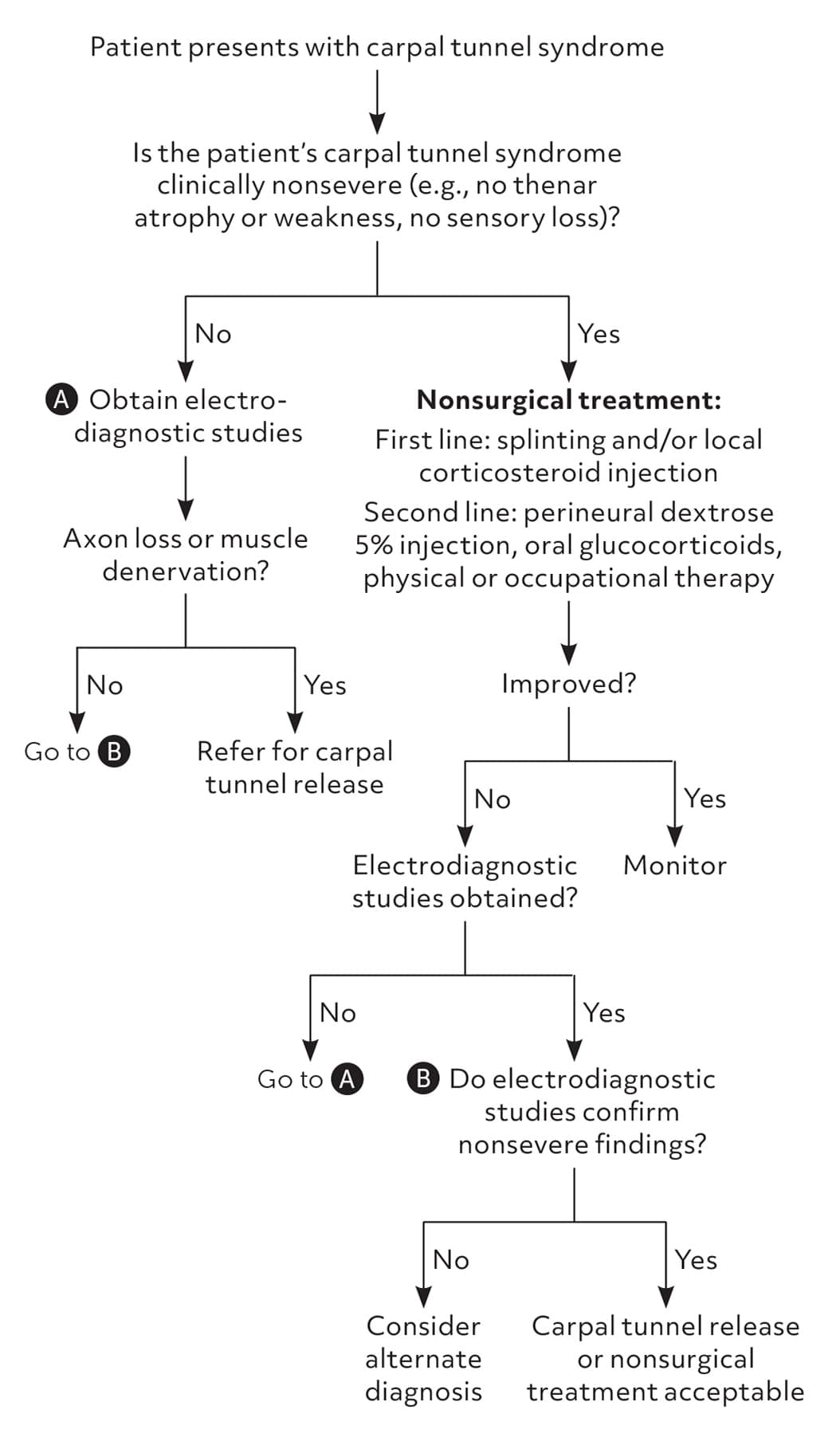
- The management of CTS is guided by clinical severity (Table 413). Up to one-half of patients with nonsevere symptoms spontaneously improve within 2 years.14 Nonsurgical treatments should be offered to patients with mild to moderate symptoms, whereas surgery is appropriate in patients with severe symptoms or signs of denervation on electrodiagnostic studies.
- Figure 2 presents a suggested approach for the treatment of CTS.
TABLE 4. Carpal Tunnel Syndrome Clinical Severity Rating
| Severity | Description |
|---|---|
| Mild | Occasional, intermittent symptoms during the day or night, including pain and paresthesia |
| Moderate | Frequent nighttime awakenings that affect sleep, frequent activity-related symptoms that do not impair function, hand clumsiness; no weakness or sensory loss on physical examination |
| Severe | Thenar atrophy, weakness of thumb abduction/opposition, constant sensory loss |
Information from reference 13.
FIGURE 2. Suggested approach for the treatment of carpal tunnel syndrome.
Splinting
- Splinting may be effective for symptom relief in patients with mild to moderate CTS and is considered first-line treatment due to accessibility, ease of use, and minimal harm.15
- Night-only splinting is as effective as continuous wear.16
- A neutral wrist splint may be more effective than an extension splint.17 The aluminum bar in over-the-counter splints can be easily straightened into a neutral position.
- Splints should be worn for at least 1 to 2 months. Symptoms usually improve within 2 weeks, and may continue to improve with up to 6 months of wear.15
Oral Medications
- Over-the-counter analgesics, such as nonsteroidal anti-inflammatory drugs and acetaminophen, have not shown benefit for CTS.4
- Short courses of prednisone (i.e., less than 2 weeks) are effective for short-term relief of symptoms but are less effective than local corticosteroid injections. Repeated or prolonged use of oral glucocorticoids are associated with serious adverse effects.18
Local Injections
- According to a Cochrane review of 14 randomized controlled trials (RCTs; N = 994), local corticosteroid injections provide significant improvement in symptoms and function at 3 months, with benefits lasting up to 6 months, and a decreased need for surgery at 1 year (number needed to treat to prevent one surgery = 7). Most trials included patients with mild to moderate CTS who were previously treated with splints.19 Higher doses may be more effective at 6 months (e.g., methylprednisolone at 80 mg vs. 40 mg vs. 20 mg). There is no significant difference among corticosteroid formulations, and combining splinting with corticosteroid injections provides no added benefit. Serious complications are rare, with no reports of neurovascular or tendon injury in the meta-analysis.19
- A systematic review of nine RCTs found that ultrasound-guided injections are more effective than landmark-guided injections; however, there was significant heterogeneity, and effect sizes were of questionable clinical significance.20
- Local corticosteroid injections provide slightly greater improvement of symptoms compared with splinting at 6 weeks, with similar outcomes at 6 months, in patients with recent onset of CTS.21
- Limited evidence suggests that a local perineural dextrose 5% injection may be effective for up to 6 months.22
Other Nonsurgical Options
- Yoga improved pain and grip strength compared with wrist splinting in an RCT of 42 patients who participated in sessions two times per week for 8 weeks.23
- Adding nerve-gliding exercises to wrist splinting does not improve outcomes.24
- Therapeutic ultrasound and carpal bone mobilization are physical and occupational therapy techniques supported by very low-quality evidence. They require multiple treatment sessions and local expertise.25
- Acupuncture has little to no short-term effect for CTS based on limited evidence.26
Surgery
- Carpal tunnel release is indicated if nonsurgical management is unsuccessful or the patient has moderate to severe symptoms and findings of nerve injury (i.e., axon loss or denervation) on electrodiagnostic studies.4
- Carpal tunnel release is effective in 70% to 90% of patients, with prognosis depending on the presence of irreversible median nerve damage.27 Serious complications occur in less than 2% of patients and include vascular, nerve, or tendon injury.27 Less than 3% of patients require repeat surgery for recalcitrant symptoms, often due to incomplete division of the transverse ligament.28
- Endoscopic and open carpal tunnel release techniques are equally effective.29 Limited evidence suggests that an endoscopic approach is less likely to result in complications, such as scarring and infection, and is associated with less postoperative pain and earlier return to work (1 week) compared with open release.28,30
- Postoperative splinting does not reduce pain or hasten recovery and may be associated with worse short-term function.4,31
- Postoperative rehabilitation is not routinely recommended due to lack of benefit.31
PROGNOSIS
- Although CTS was once thought to be a progressive disease, studies have found a significant rate of spontaneous improvement over time. One prospective cohort study that evaluated 274 hands with CTS found that after an average of 1 year, approximately 30% of nonsevere cases improved, 40% remained stable, and 20% worsened. Risk factors for progression of CTS included older age and longer duration of symptoms.32
- Splinting and local corticosteroid injections are more likely to provide long-term resolution in patients with onset of symptoms in the past 3 months and no sensory impairment on examination.33
This article updates previous articles on this topic by Wipperman and Goerl,6 LeBlanc and Cestia,34 and Viera.35
Data Sources: A PubMed search was completed in Clinical Queries using the key terms carpal tunnel syndrome, diagnosis, treatment, ultrasound, corticosteroid injection, and splinting. The search included meta-analyses, randomized controlled trials, clinical trials, and reviews. The Agency for Healthcare Research and Quality Effective Healthcare Reports, the Cochrane database, DynaMed, ACCESSS, and Essential Evidence Plus were also searched. Search dates: August 23, 2023, and May 7, 2024.
