Prostatitis is a common clinical syndrome classified into four categories: acute bacterial, chronic bacterial, chronic prostatitis/chronic pelvic pain syndrome, and asymptomatic. Bacterial prostatitis (acute and chronic) is primarily diagnosed with history and microbiologic studies, although physical examination can be helpful to localize infection within the genitourinary system. Bacterial prostatitis is treated with antibiotics; the span of treatment is guided by the duration of symptoms and presence of complications. Chronic prostatitis/chronic pelvic pain syndrome is the most common form of prostatitis and is a diagnosis of exclusion with no standardized treatments. Asymptomatic prostatitis does not require treatment and is usually diagnosed incidentally during the workup for other urologic presentations.
Prostatitis encapsulates a spectrum of clinical syndromes that affects approximately 10% to 15% of individuals assigned male at birth.1–3 It presents with varying degrees of lower urinary tract symptoms (e.g., obstructive, irritative, storage related), pelvic pain, sexual dysfunction, and systemic features. The National Institutes of Health organizes prostatitis into four categories. Categories I and II constitute 10% of cases and include acute and chronic bacterial prostatitis, respectively. Category III (chronic prostatitis/chronic pelvic pain syndrome [CPPS]) and category IV (asymptomatic inflammatory prostatitis) are noninfectious and comprise the remaining 90% of cases.4 Identifying prostatitis as bacterial (categories I and II) or nonbacterial (categories III and IV) is critical for timely treatment and appropriate antibiotic use (Table 1).5
SORT: KEY RECOMMENDATIONS FOR PRACTICE
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to https://www.aafp.org/afpsort.
TABLE 1. Evaluation and Treatment of Prostatitis
| Syndrome | Differential diagnosis | Symptoms | Physical examination | Evaluations | Treatment and management |
|---|---|---|---|---|---|
| Acute bacterial prostatitis | Acute cystitis, prostatic abscess, pyelonephritis | Genitourinary: straining, urgency, dysuria, hesitancy, frequency, obstruction, irritation Systemic: fever, malaise, arthralgia, myalgia, intense suprapubic pain, mildly to acutely ill appearance, chills, nausea, emesis, signs of sepsis (tachycardia and hypotension) | Prostate that is tender, boggy, and enlarged on digital rectal examination; distended bladder; prostate massage is not recommended | Urine culture Complete blood count with differential, electrolytes, creatinine Blood culture (if systemically unwell) | Empiric antibiotics targeting Enterobacterales while awaiting culture results* Carbapenems Ceftriaxone Fluoroquinolones Duration of treatment: ≥ 14 days Consider postvoid residual to assess underlying urinary obstruction |
| Chronic bacterial prostatitis | Benign prostatic hyperplasia, stones or foreign body within the urinary tract, bladder cancer, prostatic abscess, enterovesicular fistula | Irritative voiding symptoms; testicular, low back, or perineal pain; recurrent urinary tract infection; urethritis; epididymitis; distal penile pain | Prostate can feel normal, tender, or boggy on digital rectal examination; prostate massage can be considered for 2-glass test | Urine culture Consider 2-glass test | Fluoroquinolone (first-line), trimethoprim/sulfamethoxazole, doxycycline, fosfomycin Duration of treatment: 4 weeks if using fluoroquinolone or 6 weeks for others Consider postvoid residual to assess underlying urinary obstruction |
| Chronic pelvic pain syndrome (inflammatory and noninflammatory) | Benign prostatic hyperplasia, voiding dysfunction, bladder or prostate cancer, prostatic or müllerian duct remnants, interstitial cystitis, radiation cystitis, eosinophilic cystitis, chronic proliferative cystitis, neuropathic pain, ejaculatory duct obstruction | Chronic pelvic pain and/or sexual dysfunction and possible voiding symptoms | Abdominal and digital rectal examination to exclude underlying pathology; varying degrees of tenderness; findings are variable | National Institutes of Health-Chronic Prostatitis Symptom Index,† 2-glass test | Multimodal: combination of nonpharmacologic therapy and nonantibiotic medication |
| Asymptomatic prostatitis | — | None; incidental finding during evaluation for other conditions (e.g., infertility or elevated prostate-specific antigen level) | Not applicable | Semen analysis, prostate biopsy | No specific treatment required; treatment depends on underlying conditions and reasons for initial evaluation |
*—Selection of empiric therapy dependent on local antibiogram.
†—Used to establish diagnosis and determine treatment effect.
Adapted with permission from Sharp VJ, Takacs EB, Powell CR. Prostatitis: diagnosis and treatment. Am Fam Physician. 2010;82(4):400–401.
Bacterial prostatitis is an infection of the prostate gland. It can occur via ascending infection from the urethra, inoculation from direct manipulation of the prostate gland (e.g., biopsy), or hematogenous seeding.6 Commensal organisms within the gastrointestinal tract, particularly Enterobacterales (e.g., Escherichia coli, Klebsiella, Proteus) are the most common pathogens implicated in cases caused by ascending infection from the urethra.7 Other gastrointestinal flora, although less common, include gram-positive cocci such as Enterococcus.
Infectious prostatitis from other gram-positive cocci, such as Staphylococcus aureus and coagulase-negative staphylococci, usually occur from urinary tract manipulation (e.g., catheters) or hematogenous sources. Bacterial prostatitis after prostate biopsy is more likely caused by drug-resistant organisms due to the widespread use of prophylactic antibiotics (typically fluoroquinolones) before the procedure.8 Uncommon causes of bacterial prostatitis include Chlamydia trachomatis, Mycobacterium tuberculosis, and Burkholderia pseudomallei.9 Other organisms that less commonly cause prostatitis, such as fungi, usually occur in patients who are immunocompromised.10
Chronic prostatitis/CPPS is poorly understood, lacks universal diagnostic criteria, and is associated with negative impacts on quality of life. Asymptomatic prostatitis is usually incidentally identified during investigation for reproductive tract disorders or other urinary tract pathologies.
ACUTE BACTERIAL PROSTATITIS
Diagnosis
Pyelonephritis and acute bacterial prostatitis are recognized complications of lower urinary tract infections. Pyelonephritis occurs via microbial ascension from the lower urinary tract to the kidney, and acute bacterial prostatitis is an infection spread from the lower urinary tract to the prostate. Both syndromes are characterized by lower urinary tract symptoms (e.g., dysuria, urinary frequency and urgency, suprapubic pain) and an abrupt onset of systemic symptoms of infection (e.g., fever, chills, nausea, vomiting).
Unlike pyelonephritis, acute bacterial prostatitis typically lacks flank pain and costovertebral angle tenderness; instead, it manifests with perineal or suprapubic discomfort and urinary storage symptoms, including dribbling or hesitancy, caused by the inflamed prostate obstructing the urethral canal. Penile and scrotal pain may occur but are described less often. Pain with ejaculation may occur, although patients are typically too ill to pursue sexual activities.11
Acute bacterial prostatitis can be suspected based on these symptoms and confirmed with appropriate urine studies (e.g., urinalysis, urine culture), which can also be used to guide therapy. Bacteremia occurs as a complication of acute bacterial prostatitis in 20% of inpatient cases.12
Digital rectal examination reveals a prostate that is enlarged, boggy, and tender. Prostate massage, in which pressure is applied to the prostate during palpation, is not recommended, because it may cause bacterial seeding and subsequent clinical deterioration. Although the diagnosis of acute bacterial prostatitis can be confirmed without digital rectal examination, this practice is safe when performed gently, and it can help distinguish acute bacterial prostatitis from other conditions.7,13,14
Treatment
Treatment of acute bacterial prostatitis is similar to that of complicated urinary tract infections. Empiric antibiotic therapy is directed by local antibiogram data and severity of illness, with intravenous medications preferred in patients who are septic, hemodynamically unstable, or at risk of multidrug-resistant organisms resistant to oral antibiotics. Prostatic inflammation in acute bacterial prostatitis enhances drug penetration to prostate tissue. Oral antibiotics with effective prostate penetration (e.g., fluoroquinolones, trimethoprim/sulfamethoxazole, tetracyclines) are highly effective options if the patient is stable.15 Two weeks of antibiotic therapy is generally sufficient.7,16 Figure 1 provides an overview of diagnosis and treatment of acute bacterial prostatitis.
FIGURE 1.
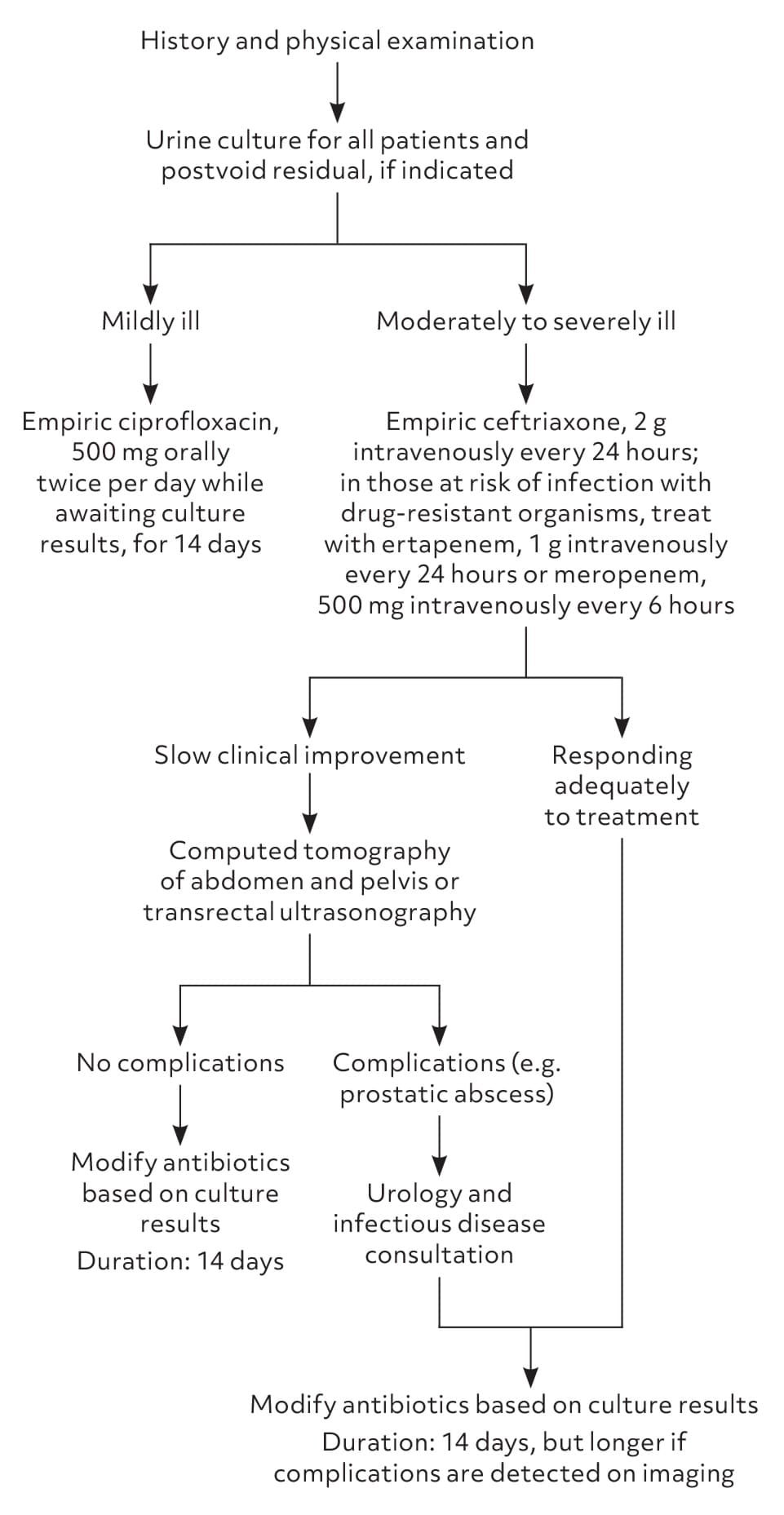
Diagnosis and treatment of acute bacterial prostatitis.
Special Considerations
Prostate abscesses occur in 3% to 6% of acute bacterial prostatitis cases and benefit from radiology-guided or surgical drainage with prolonged antibiotics in consultation with urology and infectious disease specialists.13,17 Evaluation for abscesses with transrectal ultrasonography or computed tomography should be considered in patients with higher likelihood of abscess development. This includes ill patients who require hospitalization and patients with ongoing fevers beyond 48 hours, recent urinary tract manipulation (e.g., prostatic biopsy, cystoscopy, catheterization), or relapsed symptoms despite an appropriate antibiotic course.18 Patients should also be assessed for urinary retention, which can increase the likelihood of developing prostatitis.
CHRONIC BACTERIAL PROSTATITIS
Diagnosis
Most cases of chronic bacterial prostatitis develop as primary infections, although 8% occur as a complication of acute bacterial prostatitis.6 Symptoms of chronic bacterial prostatitis mimic those of acute bacterial prostatitis, except they are more insidious and typically not associated with systemic symptoms (e.g., fever, chills, nausea, vomiting). As with acute bacterial prostatitis, additional symptoms of prostatitis are what differentiate chronic bacterial prostatitis from other urinary tract infections. The most common clinical presentation of chronic bacterial prostatitis is relapsing urinary tract infections (from the same organism) despite initial resolution of urinary symptoms with antibiotic treatment. Other diagnoses, including infected renal or bladder stones and bladder outflow obstruction (e.g., bladder diverticula, incomplete bladder emptying) are considerations with recurrent infections of the urinary tract from the same organism.
Chronic bacterial prostatitis should be suspected in patients with recurrent, episodic, and symptomatic genitourinary infections for at least 3 months.19 Palpation of the prostate may help confirm the diagnosis and is safe to perform due to the prostate being less inflamed than with acute bacterial prostatitis. The prostate may be tender or boggy, but it can also feel normal. Isolating microbial pathogens from prostatic secretions or after prostate palpation, using the Meares-Stamey 4-glass test or the modified 2-glass test, can confirm chronic bacterial prostatitis20 (Figure 25). The modified 2-glass test is most commonly used because it is easier to perform and its accuracy is similar to the Meares-Stamey 4-glass test.21 Both tests have high specificity but low sensitivity. For either test, the sensitive nature of the maneuver and the time required to conduct it are barriers for most physicians. However, these tests can help localize genitourinary infections when there is a lack of diagnostic clarity and help differentiate chronic bacterial prostatitis from noninfectious prostatitis.
FIGURE 2.
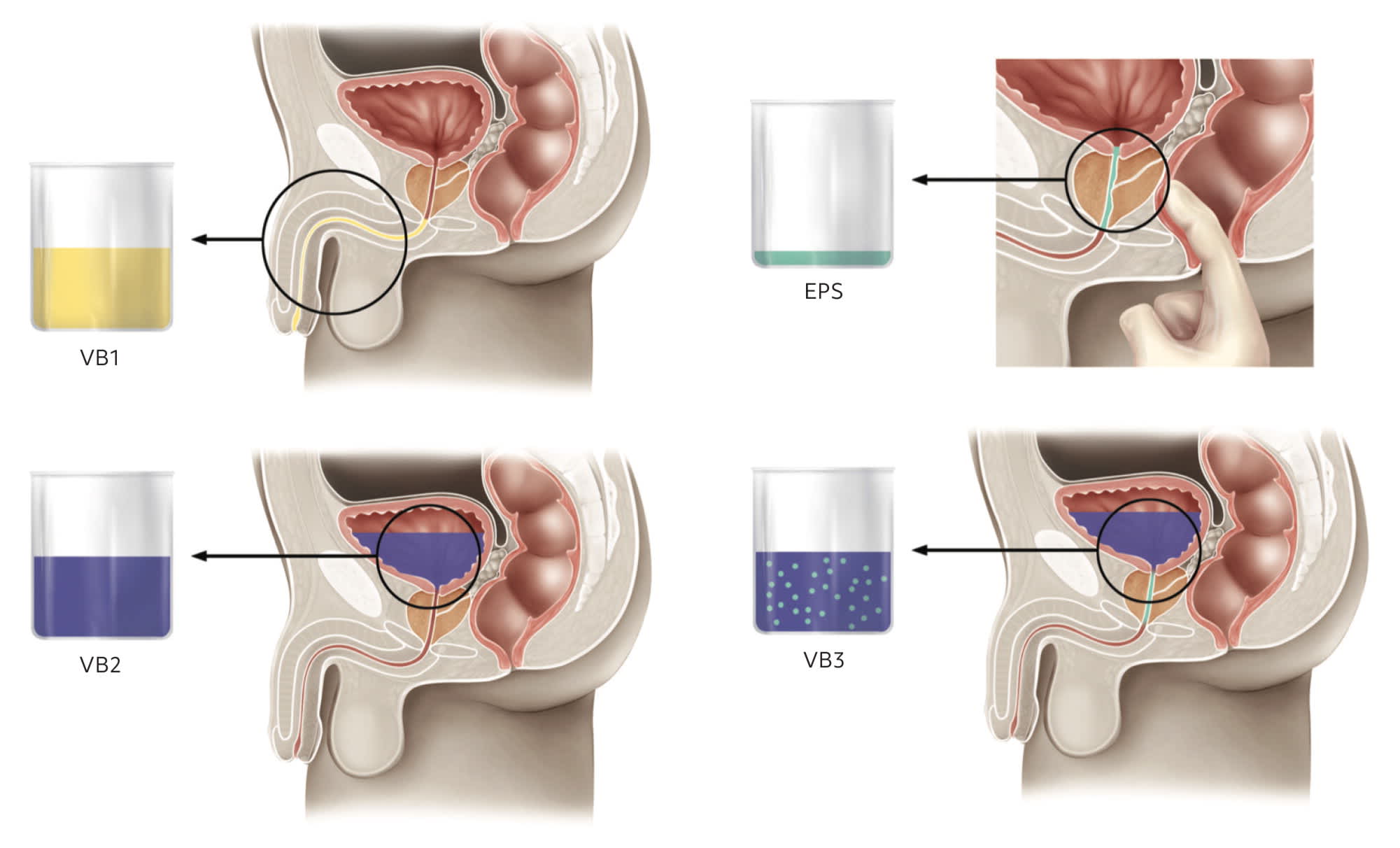
Meares-Stamey 4-glass test.
The 4-glass test is performed by sequentially collecting four separate urine samples. The first two samples represent urethral collection (VB1) and midstream urine (VB2). Subsequently, a prostate massage is performed for expressed prostatic secretions (EPS) followed by urine collection (VB3). Chronic bacterial prostatitis can be diagnosed if the bacterial colony count of the EPS or VB3 exceeds the pre-prostatic massage VB2 by 10-fold. The modified 2-glass test is performed by comparing VB2 with VB3. Prostatitis is not excluded based on the modified 2-glass test due to low sensitivity. However, specificity of the modified 2-glass test is high, with one study reporting 100% specificity.21
Illustration by Renee Cannon
Adapted with permission from Sharp VJ, Takacs EB, Powell CR. Prostatitis: diagnosis and treatment. Am Fam Physician. 2010;82(4):399.
Treatment
Treatment of chronic bacterial prostatitis includes a prolonged course (at least 3 to 6 weeks) of oral antibiotics that penetrate the alkaline environment of the chronically infected prostate. Because patients with chronic bacterial prostatitis are typically systemically well, intravenous antibiotics are reserved for patients who cannot otherwise pursue oral therapy (e.g., due to multidrug resistance). Oral therapies with the most evidence for effectiveness include fluoroquinolones, trimethoprim/sulfa-methoxazole, and doxycycline.
Fluoroquinolones are first-line agents because of their spectrum of activity against uropathogens, excellent penetration into prostatic tissue, and high oral bioavailability.22 Although supporting evidence is limited, fosfomycin is being increasingly used because of its effective prostatic penetration and effectiveness for common multidrug-resistant pathogens (e.g., extended-spectrum beta-lactamase E. coli).4 Linezolid and macrolides have reliable prostatic penetration but do not include a spectrum of activity against the most common pathogens associated with chronic bacterial prostatitis.23
Oral beta-lactams such as penicillin and cephalosporin derivatives have varying degrees of prostatic penetration with chronic bacterial prostatitis because the lack of prostate inflammation causes less favorable pharmacokinetic conditions. High-dose oral beta-lactams are being used more often to treat other deep-seated infections, such as osteomyelitis. Although evidence is lacking for the use of high-dose oral beta-lactams to treat chronic bacterial prostatitis, they may be an appropriate option if none of the other oral options mentioned can be used. Infectious disease consultation is strongly recommended before starting treatment with high-dose oral beta-lactams.
Treatment duration is 4 weeks with a fluoroquinolone and 6 weeks with other antibiotics (Table 24). Treatment duration can be extended to 12 weeks if the patient has had a prior relapse of chronic symptoms after 4 to 6 weeks of antibiotics. For patients with prostatic abscesses, source control via drainage should be pursued if possible. Antibiotics can be prolonged until repeat radiologic imaging is reassuring, or as guided by urology or infectious disease expert consultation.
TABLE 2. Pharmacologic Treatment Options for Chronic Bacterial Prostatitis
| Organism susceptibility profile | Antibiotic choices | Duration of treatment |
|---|---|---|
| Ciprofloxacin-sensitive | Ciprofloxacin, 500 mg orally twice per day or Levofloxacin, 500 to 750 mg orally once per day | 4 weeks |
| Ciprofloxacin-resistant, TMP/SMX–sensitive | TMP/SMX, 160/800 mg orally twice per day | 6 weeks |
| Ciprofloxacin-resistant, TMP/SMX–resistant, doxycycline-sensitive | Doxycycline, 100 mg orally twice per day | 6 weeks |
| Ciprofloxacin-resistant, TMP/SMX–resistant, doxycycline-resistant, fosfomycin-sensitive* | Fosfomycin, 3 g orally every 1 to 3 days | 6 weeks |
| Chlamydial prostatitis | Azithromycin, 500 mg once per day or three times per week (in the first 3 consecutive days of each week)† | 3 weeks |
| Relapsing chronic bacterial prostatitis despite adequate treatment | Antibiotics as indicated above; computed tomography of abdomen and pelvis and urologic or infectious diseases consultation also recommended | 12 weeks |
Note: Treat according to susceptibility results provided. Dosages provided are for patients with normal renal function.
TMP/SMX = trimethoprim/sulfamethoxazole.
*—Exception to susceptibility testing could be oral fosfomycin for Enterobacterales without susceptibility breakpoints (e.g., Klebsiella).
†—Doxycycline, 100 mg twice per day for 4 weeks, can also be used.
Information from reference 4.
Chronic bacterial prostatitis caused by C. trachomatis requires 3 weeks of azithromycin or 4 weeks of doxycycline.22 Prostatic infection from less common microbial causes, such as S. aureus from seeding of a disseminated infection, M. tuberculosis, or B. pseudomallei, should be treated in consultation with an infectious disease specialist. Infectious disease consultation should also be sought for treatment of immunocompromised patients.
Special Considerations
Patients with chronic bacterial prostatitis should be screened for potential causes and complications. Urinary retention predisposes individuals to recurrent genitourinary tract infections, including chronic bacterial prostatitis. It can also cause symptoms similar to chronic bacterial prostatitis (e.g., suprapubic discomfort, bladder irritation, urinary dribbling). Urinary retention can be assessed with measurement of postvoid bladder residual via ultrasonography. Ultrasonography of the urinary tract can be helpful to assess nonprostatic obstructive pathology. Additional imaging with computed tomography or transrectal ultrasonography is typically reserved for patients with suspected complications, such as prostatic abscess.17,18 The use of prostate-specific antigen as a marker to predict relapse is not validated.7
CHRONIC PROSTATITIS/CHRONIC PELVIC PAIN SYNDROME
Diagnosis
Chronic prostatitis/CPPS is a diagnosis of exclusion, characterized by pelvic pain with or without urinary symptoms or sexual dysfunction (e.g., ejaculatory pain, premature ejaculation, erectile dysfunction) for 3 of the preceding 6 months. Despite the nomenclature, the prostate's role in these symptoms is unclear.24
Chronic prostatitis/CPPS is diagnosed by excluding diseases with similar presentations, such as bacterial prostatitis, renal stones, orchitis, inguinal lymphadenopathy, or abdominal hernias.25 The National Institutes of Health-Chronic Prostatitis Symptom Index is a validated tool to assess symptoms and quality of life in patients with the condition.26 Examination may reveal myofascial tenderness of the pelvic floor with varying degrees of prostate tenderness. Urinalysis and urine culture testing may identify leukocytes in the urine after prostate massage. Importantly, hematuria and an elevated prostate-specific antigen level should not be ascribed to chronic prostatitis/CPPS.27 Referral to urology for further workup (e.g., cystoscopy, urodynamic studies) may be required.
Treatment
To guide treatment, the UPOINT phenotype system categorizes individuals into six domains: urinary, psychosocial, organ specific, infectious, neurologic/systemic, and tenderness of skeletal muscles.26 A variety of medications, including antibiotics, anti-inflammatories, alpha blockers, 5-alpha reductase inhibitors, antidepressants, and neuroleptics have been tested with varying success.24,27 Antibiotic therapy has not been shown to be superior to placebo for chronic prostatitis/CPPS.28 Some patients describe benefit from antibiotics, but it is likely from the anti-inflammatory properties of those medications. Antibiotics are not recommended without proven infection.24
Nonpharmacologic therapies, including physiotherapy, acupuncture, and cognitive behavior therapy, have varying degrees of effectiveness for chronic prostatitis/CPPS and continue to be studied.29–31 A multidisciplinary approach with urology, pain specialists, and allied health professionals should be considered for treatment.
ASYMPTOMATIC PROSTATITIS
Asymptomatic prostatitis is usually diagnosed incidentally when inflammatory cells are identified on semen analysis or prostate biopsy during evaluation for other entities. No specific treatment or evaluation is necessary, and any further workup is directed by the primary urologic symptom.14,32 The condition's prognostic value is unclear.
This article updates previous articles on this topic by Holt, et al.33; Coker and Dierfeldt13; Sharp, et al.5; and Stevermer and Easley.34
Data Sources: A PubMed search was completed in Clinical Queries using the key terms acute prostatitis and chronic prostatitis. The search included meta-analyses, randomized controlled trials, clinical trials, observational studies, and reviews. The Agency for Healthcare Research and Quality Effective Healthcare Reports, the Cochrane database, DynaMed, and Essential Evidence Plus were also searched. Search date: May 11, 2024.
