Long-acting reversible contraceptives (LARCs), including intrauterine devices (IUDs) and etonogestrel single rod implants, are effective in preventing unintended pregnancy. In the post-Dobbs era, it is important for family physicians to expand access to LARCs because previous research has shown a decline in LARC use in abortion restrictive states.1
A 2019 report indicated that although LARC provision continued to rise, less than one-fourth of family physicians provided IUDs or implants.2 A 2021 Health Resources and Services Administration report found that obstetrician-gynecologists will provide only 51% of women's health services needed in non-metropolitan areas by 2030.3 This analysis shows how rates of LARC provision have evolved among family physicians and identifies the impact of practice location on the likelihood of providing contraceptive care.
The authors analyzed responses to the American Board of Family Medicine Continuing Certification Examination Registration Questionnaire from 14,004 family physicians (Figure 1). A descriptive cross-sectional analysis by year between 2018 and 2022 was completed, with a demographic assessment of physicians who were more likely to provide LARCs, including patient panel composition and rurality. Rurality was determined by Rural Urban Commuting Area codes greater than 5.4 The percentage of family physicians who offered IUDs or implants increased from 23.9% in 2018 to 30% in 2022. The number of family physicians who provided implant insertion increased from 12.9% to 20.8%; those who provided IUDs also increased from 22.9% to 25.5%. Family physicians whose patient panels contained a higher proportion of female patients 5 to 18 years of age were most likely to provide LARCs (P < 0.01).
FIGURE 1.
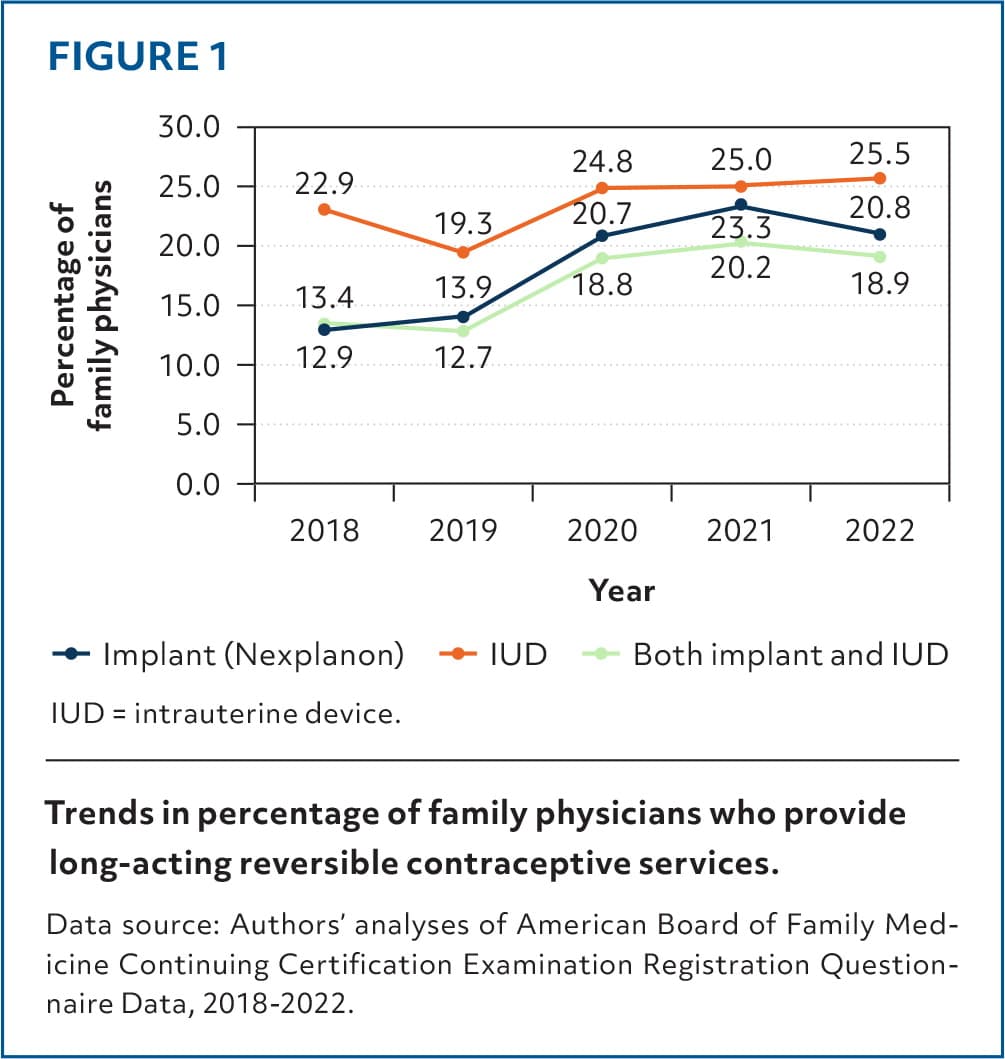
Trends in percentage of family physicians who provide long-acting reversible contraceptive services.
Data source: Authors' analyses of American Board of Family Medicine Continuing Certification Examination Registration Questionnaire Data, 2018–2022.
The percentage of family physicians providing LARC services increased as the remoteness of practice setting increased (P < 0.01). A higher percentage of rural family physicians (37%) provided implants or IUDs in their practice compared with their urban colleagues (24.7%).
Given the continued state restrictions on patients' reproductive rights in the United States, access to LARCs is increasingly important. Individuals in rural areas have less access to obstetrician-gynecologists and higher visit rates to family physicians than those in urban areas.5 LARC provision by family physicians is critical in rural areas, where family planning services are less available to patients than in urban areas.6 However, given the low absolute number of family physicians who provide these contraceptive options, more progress is needed to adequately meet the needs of patients.
Family medicine residency programs must continue to provide comprehensive LARC training. Because many residents feel competent to provide LARCs upon graduation but do not continue using this skill, further research is needed to identify barriers to provision.7 Advocating for payment models that incentivize LARC procedures and continued policy development to support family physicians' broad scope of practice is essential to ensure patient access to protection from unintended pregnancies.
