In many parts of the United States, only one primary care physician per 2,000 people is available.1 Although the ideal panel size has not been determined, an estimated reasonable size is 1,200 to 1,400 people per full-time physician.2 This shortage is expected to worsen in the next decade with population growth, stagnation in training opportunities, and increased medical complexity of the aging population. Producing new primary care physicians relies on federal funding for family, pediatric, geriatric, and internal medicine residency positions. Investment in primary care residencies and the creation of residency positions in areas with high need are essential because more than one-half of graduates from primary care residencies practice within 100 miles of where they trained.3 Areas with a shortage also tend to be regions with high social deprivation and worse medical outcomes, therefore requiring more resources and physician care.4 Although the need for primary care physicians is clear, the relationship between graduate medical education (GME) spending and producing new primary care physicians is not well studied.
Using several databases, the association between the Medicare GME funding distributed to each state, in millions of dollars per 100,000 people, and the percentage of new physician workforce entering primary care after 5 years were compared. In this study, primary care physician is defined as a graduate of any of the following residencies or fellowships—family, pediatric, geriatric, or internal medicine—assuming that all graduates entered primary care and recognizing that internists and pediatricians often subspecialize. Hospitalists were excluded. Total GME funding was found to be inversely related to new primary care physicians.
Figure 1 shows northeastern states receive high GME funding but produce a relatively low number of primary care physicians. Generally, southern states receive relatively low GME funding and produce a small number. Northwestern states receive low GME funding but produce a relatively higher number of primary care physicians (70.8) compared with the national average (69.8) of primary care physicians per 100,000 people. This number is still low compared with Canada, which averages 119 primary care physicians per 100,000 people.5
FIGURE 1.
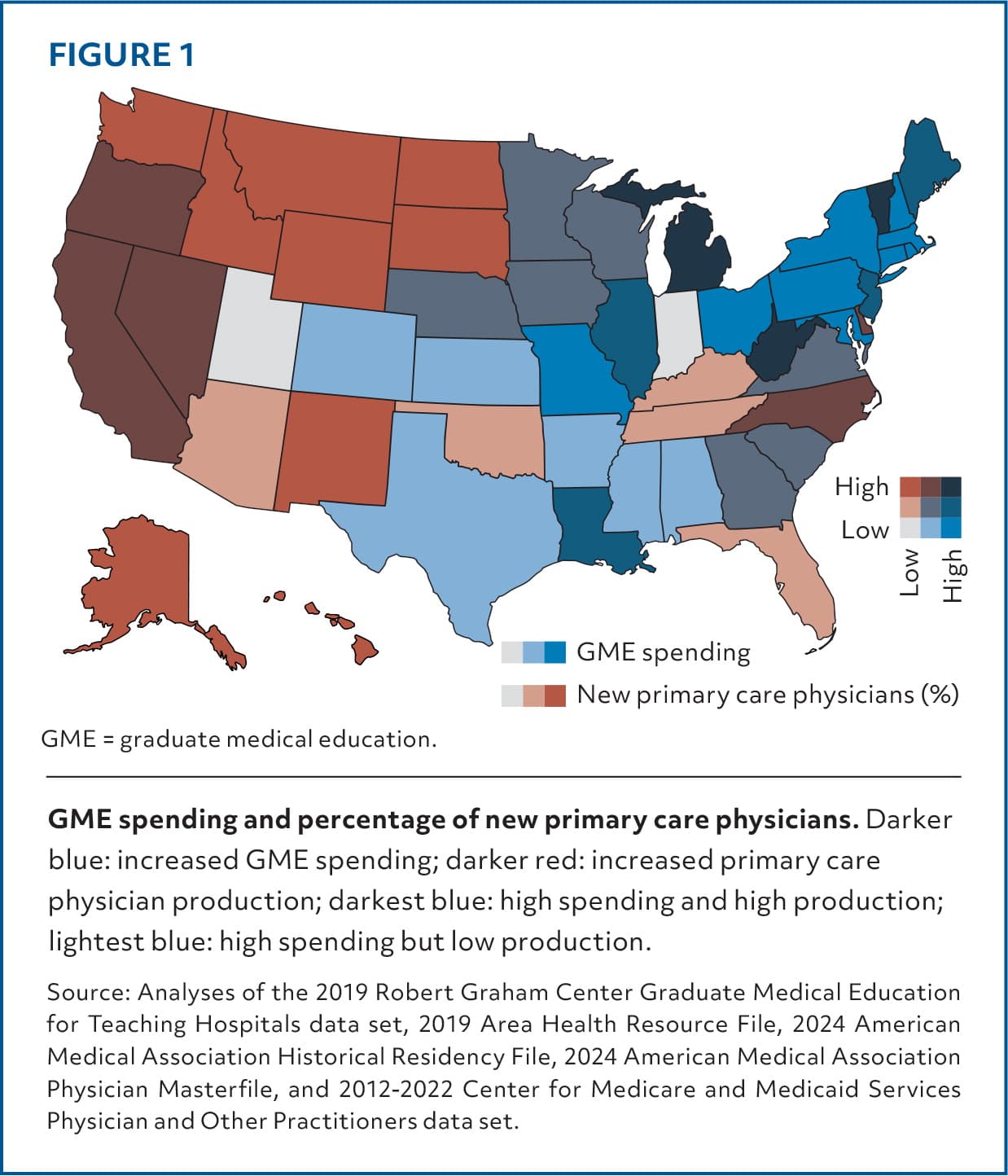
Source: Analyses of the 2019 Robert Graham Center Graduate Medical Education for Teaching Hospitals data set, 2019 Area Health Resource File, 2024 American Medical Association Historical Residency File, 2024 American Medical Association Physician Masterfile, and 2012–2022 Center for Medicare and Medicaid Services Physician and Other Practitioners data set.
These estimates of output are likely inflated because only 9.4% of internal medicine graduates intend to practice primary care after residency and approximately 54% of pediatric residents remain in primary care.6,7 In 2022, only 24.4% of all physicians entered primary care (as defined previously), and even in states with a ratio of high GME spending to producing primary care physicians (eg, North Dakota), only 43% remain in primary care.8
A multipronged approach to direct GME dollars toward primary care is needed. New funding for residencies should mandate a threshold of approximately 30% to 50% of new positions allocated to primary care specialties commensurate with other high-income countries.9 GME funding should be distributed equitably to meet the needs of the health care system. Publicly available accountability measures should be implemented to track and report GME funding to prioritize long-term retention. The inverse association between GME spending and producing a family physician indicates that such disbursement currently incentivizes production of higher-paid subspecialists; closing the reimbursement disparity for primary care specialties is necessary. Federal mandates, accountability, and more equitable reimbursement policies could improve the production of primary care physicians while continuing to train other specialists.
