Nausea and vomiting are common symptoms that can reduce quality of life and indicate life-threatening illness. Acute nausea and vomiting last up to 7 days. In the absence of alarm symptoms, they are typically treated symptomatically and without an extensive evaluation. Typical causes include gastroenteritis or other viral syndromes, foodborne illness, acute migraine headaches, vestibular disturbances, early pregnancy, and adverse effects of medication. Chronic nausea and vomiting last 4 weeks or longer and have a broad differential diagnosis. Causes can be gastrointestinal, infectious, metabolic, neurologic, psychiatric, or related to medications and toxins. A careful history of related factors is essential to guide the initial evaluation and narrow the differential diagnosis. These factors include associated symptoms, timing of onset and duration of symptoms, exacerbating or relieving factors, alarm symptoms, medication and substance use, relationship with recent food ingestion, and comorbidities. Nonpharmacologic management options include fluid and electrolyte replacement; small, frequent meals; and avoidance of trigger foods. Antiemetic drugs effectively reduce symptoms of acute nausea and vomiting, but chronic symptoms are often more challenging to treat. When a specific etiology is not identified, a serotonin antagonist or dopamine antagonist can be used. However, medications may also target the suspected cause of symptoms and the neurotransmitters involved in central and peripheral pathways of nausea and vomiting. Pharmacologic therapy should be used for the shortest time necessary to control symptoms.
Nausea and vomiting are common symptoms that lead patients to visit family physicians. Although usually self-limiting, they are significant causes of reduced quality of life and can indicate life-threatening illness.1,2
SORT: KEY RECOMMENDATIONS FOR PRACTICE
| Clinical recommendation | Evidence rating | Comments |
|---|---|---|
| In the absence of alarm symptoms, acute nausea and vomiting should be treated symptomatically without an extensive evaluation.2,4,5 | C | Expert opinion, usual practice |
| Although serotonin antagonists are commonly used for acute gastroenteritis, the evidence to support their use in adults is limited.33,34 | C | Expert opinion, usual practice; systematic review of low-quality studies with insignificant results |
| Metoclopramide in combination with aspirin should be considered for nausea and vomiting caused by acute migraine.35 | A | Meta-analysis of good-quality randomized controlled trials |
| Antihistamines and anticholinergics can be used for motion sickness symptoms.41,42 | B | Meta-analysis of randomized controlled trials |
| Pyridoxine alone or combined with doxylamine is a first-line option for nausea and vomiting in pregnancy.21 | C | Consensus guidelines supported by systematic reviews with inconsistent findings |
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to https://www.aafp.org/afpsort.
Nausea is the unpleasant sensation that vomiting might occur, whereas vomiting is the forceful expulsion of gastric contents from the mouth. Vomiting should be distinguished from regurgitation, the involuntary reflux of gastric contents into the esophagus and sometimes mouth without abdominal wall contractions, and from rumination, which is the voluntary, effortless flow of gastric contents into the mouth, where they are typically rechewed and swallowed. Retching involves spasmodic contractions with a closed glottis; it often precedes vomiting.3
Acute nausea and vomiting last up to 7 days. In the absence of alarm symptoms or other clinical clues warranting investigation (Table 12,4 ), they are typically self-limiting and treated symptomatically without an extensive evaluation.5 However, symptoms or physical examination findings suggestive of moderate to severe dehydration or a surgical condition require further evaluation, often in the emergency department.2,6 In comparison, chronic nausea and vomiting persist for 4 weeks or longer. Chronic symptoms have a broad differential diagnosis, including gastrointestinal (GI) and other causes, and are often more challenging to treat.
TABLE 1. Alarm Symptoms and Signs for Concern in Adults With Nausea and Vomiting
| History | Physical examination |
|---|---|
| Age > 55 years Change in bowel habits Early satiety Feculent vomiting Persistent vomiting Progressive dysphagia Severe abdominal pain Unintended weight loss > 5% | Acute abdomen Altered mental status Evidence of gastrointestinal bleeding Focal neurologic deficit Jaundice Palpable abdominal mass |
Initial Evaluation
A careful history of related factors is essential to guide the initial evaluation and narrow the differential diagnosis, although the patient report may not be well-defined. These factors include associated symptoms; alarm symptoms, such as unintentional weight loss or progressive dysphagia; medication and substance use; relationship with recent food ingestion; exacerbating or relieving factors; timing of onset and duration of symptoms; and comorbidities. Certain characteristic presentations of nausea and vomiting suggest a particular diagnosis or the next diagnostic step (Table 24,7–12 ).
TABLE 2. Presentations of Nausea and Vomiting That Suggest Specific Diagnoses
| Clinical presentation | Suggested diagnosis | Suggested tests |
|---|---|---|
| Acute onset | Gastroenteritis, medication-related effect, cholecystitis, pancreatitis | Cholecystitis: right upper quadrant ultrasonography 7 Pancreatitis: lipase level, ultrasonography to assess for gallstones, contrast-enhanced abdominal CT in patients with severe illness8 |
| Associated with diarrhea, headache, fever, and myalgia | Viral gastroenteritis | None |
| Bilious vomiting | Small bowel obstruction | CT9 |
| Continuous vomiting | Conversion disorders | Electrolyte levels |
| Delayed vomiting (more than 1 hour after meals) | Gastric outlet obstruction, gastroparesis | Obstruction: abdominal radiography or CT10 Gastroparesis: gastric emptying study11 |
| Feculent or foul odor | Intestinal obstruction | CT9 |
| Habitual postprandial and irregular vomiting | Major depression | Patient Health Questionnaire-9, Beck Depression Inventory |
| Insidious onset | Gastroesophageal reflux disease, gastroparesis, metabolic disorder, pregnancy | Gastroesophageal reflux disease: EGD if alarm signs are present or condition does not improve with empiric therapy Gastroparesis: gastric emptying study11 Metabolic disorders: serum chemistries, thyroid-stimulating hormone, chest radiography Pregnancy: pregnancy test in patients of childbearing potential, with pelvic ultrasonography if ectopic pregnancy suspected |
| Patient reports previous organic or functional gastrointestinal illness | Chronic psychogenic vomiting | Electrolyte levels, further evaluation if organic cause suspected |
| Projectile vomiting | Intracranial disorders, increased intracranial pressure, gastric outlet obstruction | Brain CT or MRI12 |
| Regurgitation of undigested food | Achalasia, esophageal stricture, Zenker diverticulum | EGD, upper gastrointestinal barium study |
| Vomiting before breakfast | Alcohol ingestion, increased intracranial pressure, pregnancy, uremia | Increased intracranial pressure: brain CT or MRI12 Pregnancy: pregnancy test in patients of childbearing potential, with pelvic ultrasonography if ectopic pregnancy is suspected Uremia: renal function testing, electrolyte levels |
| Vomiting during or soon after meals | Anorexia nervosa, bulimia nervosa | Electrolyte levels |
| Vomiting partly digested food | Gastric outlet obstruction (without bile), gastroparesis | Obstruction: abdominal radiography |
CT = computed tomography; EGD = esophagogastroduodenoscopy; MRI = magnetic resonance imaging.
A detailed physical examination can help identify negative consequences of vomiting such as dehydration (e.g., dry mucous membranes, skin tenting, orthostatic hypotension) or weight loss that might require laboratory evaluation or fluid replacement. Specific diagnostic clues may also be present. Diabetic ketoacidosis can present with altered mental status and fruity odor to the breath. Hyperpigmentation raises concern for Addison disease, whereas tremor or lid lag could indicate thyrotoxicosis. Nystagmus or postural instability may be seen in vestibular dysfunction. The abdominal examination is important in localizing a GI etiology or identifying a surgical emergency; attention should focus on localized tenderness or signs of peritoneal inflammation, such as rebound tenderness or pain with even gentle movement of the abdomen or pelvis. Further evaluation is also warranted in the presence of abnormal bowel sounds and any masses, organomegaly, or ascites.
Differential Diagnosis
Causes of nausea and vomiting can be considered by etiologic category: GI, infectious, medications and toxins, metabolic, neurologic, psychiatric, syndromic, or other (Table 32,4,5,13–16 ).
TABLE 3. Differential Diagnosis of Nausea and Vomiting in Adults
| Common causes | Uncommon causes | |
|---|---|---|
| Gastrointestinal | Appendicitis Cholecystitis Cholelithiasis Dyspepsia Gastritis Gastroesophageal reflux disease Gastroparesis Irritable bowel syndrome Peptic ulcer disease | Adhesions Esophageal motility disorders Incarcerated hernia Intestinal obstruction Mesenteric ischemia Pancreatitis Peritonitis |
| Infections | Bacterial gastroenteritis Foodborne illness Pyelonephritis Viral gastroenteritis | Brain abscess Encephalitis Meningitis Pneumonia |
| Metabolic | Chronic renal insufficiency Diabetic ketoacidosis Electrolyte abnormalities Pregnancy | Adrenal disorder Parathyroid disorder Thyroid disorder |
| Medications and toxins | Antibiotics Chemotherapy Excessive ethanol Glucagon-like peptide-1 receptor agonists Levodopa Marijuana Metformin Nonsteroidal anti-inflammatory drugs Opiates Oral contraceptives and other estrogens | Anesthetics Antiarrhythmics Anticonvulsants Organophosphates and pesticides Radiation therapy |
| Neurologic | Benign paroxysmal positional vertigo Migraine Motion sickness Pain | Cerebrovascular event Closed head injury Hydrocephalus Idiopathic intracranial hypertension Intracranial mass Meniere disease Seizure disorder |
| Psychiatric | Anxiety Depression Eating disorder | |
| Syndromes | Cannabinoid hyperemesis syndrome Chronic nausea and vomiting syndrome Cyclic vomiting syndrome | |
| Other | Acute myocardial infarction Nephrolithiasis | Acute glaucoma |
GASTROINTESTINAL
GI disorders commonly cause nausea and vomiting. Acute symptoms are most often due to an infectious etiology, an inflammatory process (e.g., appendicitis, cholecystitis, pancreatitis), or an obstruction of the gastric outlet or intestines. Gastroparesis and other motility disorders are more likely to present with chronic symptoms and have an insidious onset.11 Chronic nausea and vomiting may occasionally be secondary to dyspepsia, gastroesophageal reflux disease, peptic ulcer disease, or irritable bowel syndrome.17
INFECTIOUS
The most common cause of acute nausea and vomiting is viral gastroenteritis, followed by foodborne illness. Viral gastroenteritis is typically caused by norovirus, adenovirus, or rotavirus. Symptoms often include fever, diarrhea, and mild abdominal pain, but no significant abdominal tenderness. These infections are typically self-limiting.6 Other viral infections such as COVID-19 can also present with nausea and vomiting.18 Foodborne illness presents with vomiting or diarrhea and may be caused by numerous bacterial pathogens, including Escherichia coli (enterotoxigenic or Shiga toxin–producing), Staphylococcus aureus endotoxin, Campylobacter, Salmonella, Clostridium perfringens, Toxoplasma gondii, and Listeria monocytogenes. When identified, these infections should be reported to local health agencies.19 Acute nausea and vomiting are also commonly seen in infections of the genitourinary tract, the upper and lower respiratory systems, and the central nervous system. An infectious etiology may be suggested by fever and focal symptoms at the site of infection, in addition to nausea and vomiting.
MEDICATIONS AND TOXINS
Numerous medications cause nausea and vomiting, most often within days of initiation. Common examples include antibiotics (especially macrolides and sulfonamides), chemotherapeutics, nonsteroidal anti-inflammatory drugs, opiates, metformin, glucagon-like peptide-1 receptor agonists, and non-prescription drugs. Intoxication or withdrawal from alcohol may also cause nausea and vomiting.
METABOLIC AND ENDOCRINE
Pregnancy is the most common endocrine cause of nausea and vomiting; up to 75% of pregnancies have recurrent symptoms. The diagnosis should be considered in patients with childbearing potential, especially before imaging is obtained. Hyper-emesis gravidarum—persistent vomiting in pregnancy unrelated to other causes—often results in weight loss and evidence of acute starvation (e.g., ketonuria); it is limited to 0.5% to 1% of pregnancies.20,21 Other metabolic etiologies include acidosis and thyroid, parathyroid, and adrenal disorders. Uremia and electrolyte disorders such as hyponatremia, hypokalemia, and hypercalcemia may also present with nausea and vomiting.
NEUROLOGIC
Nausea and vomiting may be caused by any process that increases intracranial pressure, including hydrocephalus, space-occupying lesions, hemorrhage, and idiopathic intracranial hypertension. Labyrinthine disorders such as benign paroxysmal positional vertigo, vestibular neuritis, and Meniere disease are peripheral neurologic causes of nausea and vomiting that are often accompanied by vertigo.22 Motion sickness, which can result from a mismatch between visual cues suggesting a person is stationary and the vestibular system detecting motion, is another possible cause. Migraine headaches are commonly accompanied by nausea with or without vomiting.
PSYCHIATRIC
Anxiety and depression may present with nausea and vomiting. Rarely, a factitious disorder can also have these symptoms. Eating disorders such as anorexia nervosa and bulimia nervosa do not typically present with vomiting as a reported symptom, and it may be denied even when present, but affected patients may require assessment and treatment for related complications.23
SYNDROMIC
The Rome IV criteria describe three functional disorders of nausea and vomiting (known as syndromes) that have a prevalence of approximately 3% in the United States.15 Chronic nausea vomiting syndrome requires the occurrence of bothersome symptoms weekly for at least 3 months. It can be diagnosed in the absence of an eating disorder or organic, metabolic, systemic, or psychiatric etiology after an investigation that includes upper endoscopy.
Cyclic vomiting syndrome presents with discrete, recurrent episodes of vomiting classically involving a prodrome of nausea and sometimes concurrent symptoms such as panic, diarrhea, and diaphoresis. This is followed by a vomiting phase that lasts up to a week and may include migraine-like symptoms, but no other vomiting between episodes.
Cannabinoid hyperemesis syndrome is increasing in prevalence as cannabis becomes more widely available and can contain higher amounts of tetrahydrocannabinol. Presentation is similar to cyclic vomiting syndrome, and the condition is associated with significant, prolonged cannabis use (typically multiple times per day for more than 2 years) and relief after sustained cessation.24 There is controversy regarding the diagnostic criteria for cannabinoid hyperemesis syndrome and whether it is a distinct syndrome or a subset of cyclic vomiting syndrome. Both conditions are often associated with taking prolonged hot showers or baths to relieve symptoms.15,16,25–27
Laboratory Studies and Imaging
When indicated by the history and physical examination, initial laboratory studies should include a basic or comprehensive metabolic panel and complete blood count (Figure 14,5,12,20,23,27 ). Other directed tests, such as measurement of thyroid-stimulating hormone, urinalysis, or a pregnancy test when evaluating patients of childbearing potential, may also be warranted to confirm a diagnosis suggested by the history and physical examination. Lipase testing can be considered if pancreatitis is in the differential diagnosis. Measurement of C-reactive protein can help identify an inflammatory process. Urine drug screening or testing of serum drug levels can detect drug toxicity; examples include elevated acetaminophen level or the presence of opioids or cannabis. Additionally, intestinal bacterial or parasitic infections suspected in prolonged cases may be identified via stool testing.20
FIGURE 1.
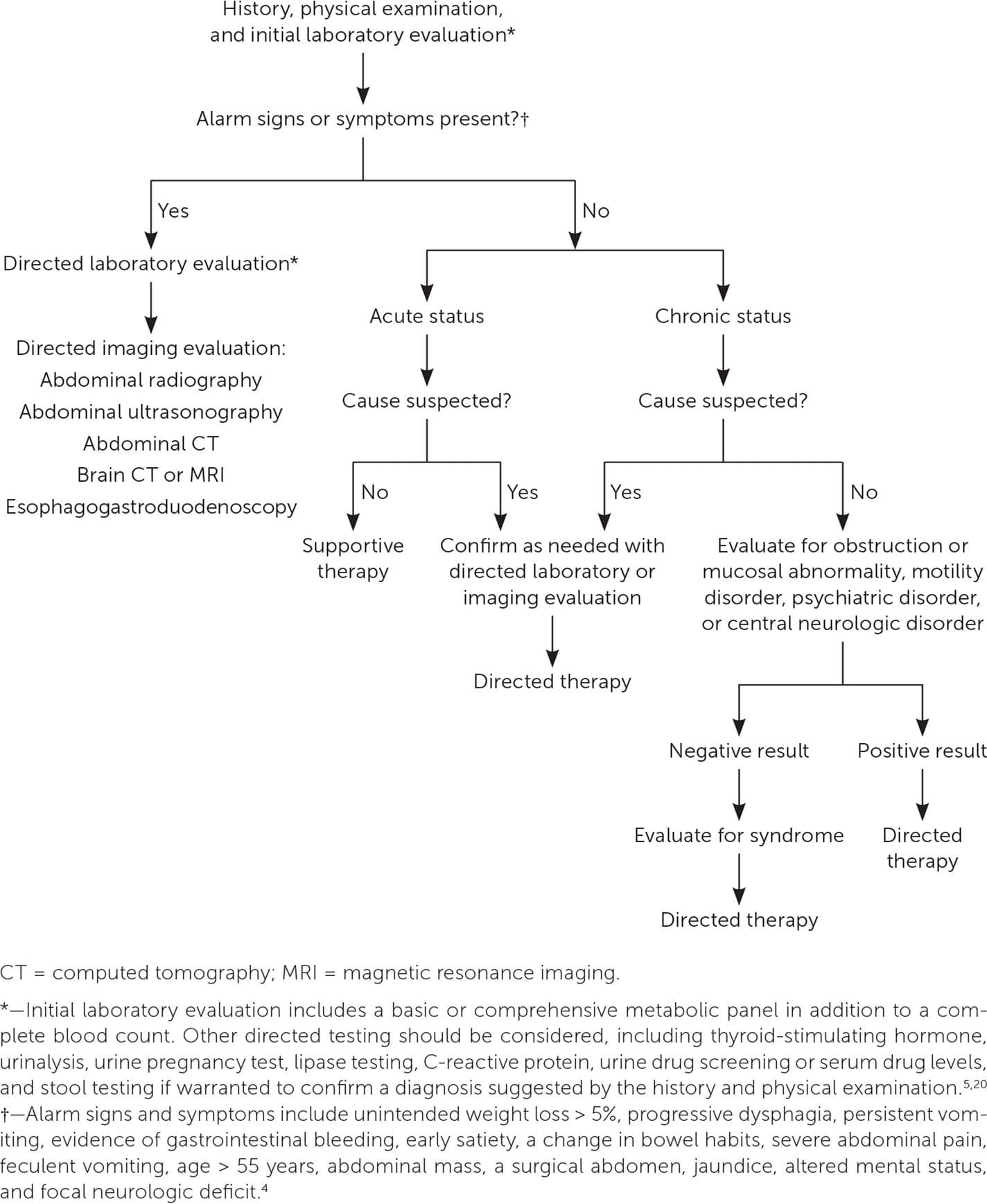
Evaluation of nausea and vomiting in adults.
Imaging evaluation is determined by the suspected diagnosis. Abdominal radiography or computed tomography is indicated for possible obstruction. Ultrasonography is the first-line imaging study if gallstones are suspected or if imaging is needed during pregnancy.7 When signs suggest ulcer or refractory gastroesophageal reflux disease, esophagogastroduodenoscopy should be considered. Computed tomography commonly identifies nephrolithiasis.9 If a central cause is suspected, imaging of the head should be performed.12
If there is no evidence of an obstruction or a mucosal disorder, and nausea and vomiting persist in conjunction with postprandial fullness, a gastric emptying study can identify motility disorders such as gastroparesis with delayed gastric emptying of solids.11
Management
When alarm symptoms are not present, treatment of nausea and vomiting can be supportive or directed at a suspected etiology based on histor y and physica l examination. In the case of acute nausea and vomiting, symptoms are typically self-limiting, and supportive therapy may be adequate without further evaluation. Nonpharmacologic management should include fluid and electrolyte replacement, if indicated, with small, frequent meals and avoidance of trigger foods.20 Medications may be used for symptom relief. Chronic nausea and vomiting related to gastroesophageal reflux disease or dyspepsia are often treated empirically with an acid-blocking medication; however, subacute or chronic symptoms may require further evaluation.
Several classes of medications are available to treat nausea and vomiting (Table 44,5,13,28–30 ). In the absence of a clear etiology, a general approach may include a serotonin antagonist or dopamine antagonist.13,28 Otherwise, medication should target neurotransmitters likely to be involved in afferent pathways leading to activation of the vomiting center in the medulla.5,28–30 The cost of medications and potential for adverse effects are also important considerations. Generally, medications are used in the short term to relieve symptoms. Although there are formal guidelines for using medications to prevent postoperative or chemotherapy-induced nausea and vomiting, an in-depth discussion of these topics is beyond the scope of this review. Rather, this section focuses on medications commonly used in the primary care setting.
TABLE 4. Common Medications for the Treatment of Nausea and Vomiting in Adults
| Medication | Dosage | Common uses | Common adverse effects |
|---|---|---|---|
| Antihistamines and anticholinergics | |||
| Dimenhydrinate Diphenhydramine Meclizine Scopolamine | 50 mg every 6 hours 25 mg every 6 hours 25 mg every 6 hours One patch every 3 days | Vertigo, motion sickness | Sedation, blurred vision, dry mouth, urinary retention, constipation |
| Dopamine antagonists | |||
| Metoclopramide Prochlorperazine Promethazine | 10 mg four times daily 5 to 10 mg every 6 hours 12.5 to 25 mg every 6 hours | Acute gastroenteritis, migraine, gastroparesis (metoclopramide) | Sedation, extrapyramidal symptoms, hypotension, prolonged QT interval |
| Serotonin antagonists | |||
| Ondansetron | 4 mg every 8 hours | Acute gastroenteritis, pregnancy-induced nausea | Headache, constipation, prolonged QT interval |
| Other agents | |||
| Doxylamine/pyridoxine (Bonjesta, Diclegis) | 1 to 2 tablets per day | Pregnancy-induced nausea | Sedation |
| Ginger | 250 mg four times daily | Migraine, pregnancy-induced nausea | — |
| Pyridoxine | 10 to 25 mg three or four times daily | Pregnancy-induced nausea | Paresthesia, somnolence |
Note: All medications listed are available at low cost (no more than a few dollars per day).
Serotonin mediates central activation of the chemoreceptor trigger zone and visceral stimulation in the GI tract. Based on a recent study in children, serotonin antagonists can be used to treat nausea and vomiting caused by acute gastroenteritis.31 A Cochrane review of randomized controlled trials (RCTs) also found that oral ondansetron effectively reduces vomiting in children with acute gastroenteritis.32 However, evidence regarding the use of these agents in adults with acute gastroenteritis is limited.33,34
Like serotonin, dopamine leads to activation of the vomiting center. Dopamine antagonists such as prochlorperazine and promethazine have also been used for gastroenteritis, although there is similarly a lack of quality evidence for their effectiveness.33,34 Dopamine antagonists may be helpful in treating nausea and vomiting caused by acute migraine headaches, because dopamine is established as a primary mediator of nausea and vomiting in this scenario. A Cochrane review of RCTs found that patients with acute migraine headaches who were treated with metoclopramide in addition to aspirin had significantly less nausea and vomiting than those receiving aspirin alone.35
Dopamine antagonists are also used to treat chronic nausea and vomiting related to gastroparesis. A network meta-analysis of RCTs found a small benefit of metoclopramide for nausea and bloating.36 Metoclopramide is an antiemetic and a prokinetic agent that accelerates gastric emptying.37 The American College of Gastroenterology recommends use of a small particle diet with metoclopramide for refractory gastroparesis symptoms; however, this is based on low-quality evidence.38 Due to the risk of extrapyramidal effects, including tardive dyskinesia, the duration of treatment with metoclopramide should be limited to 12 weeks. Haloperidol is another dopamine antagonist with similar adverse effects.29 A Cochrane review of published RCTs concluded that there is insufficient evidence to determine the effectiveness of haloperidol for nausea and vomiting in palliative care.39
Histamine and acetylcholine are mediators of nausea and vomiting caused by a vestibular process. Antihistamines such as meclizine and diphenhydramine are often used as vestibular suppressants for vertigo and associated motion sickness; however, treatment should be short term and limited to patients with severe symptoms due to potential adverse effects, especially in older adults.40 Dimenhydrinate is another antihistamine that prevents motion sickness symptoms more effectively than placebo but causes more sedation.41 Scopolamine is an anticholinergic agent that prevents nausea and vomiting from motion sickness more effectively than placebo and similarly to antihistamines, but with less drowsiness.42
MANAGEMENT IN PREGNANCY
The neurotransmitters involved with nausea and vomiting in early pregnancy are unknown. A variety of medications as well as complementary and alternative therapies have been tried to alleviate symptoms. The American College of Obstetricians and Gynecologists recommends vitamin B6 (pyridoxine) alone or in combination with doxylamine as first-line pharmacologic therapy.21 Two formulations of combined doxylamine/pyridoxine (Diclegis and Bonjesta) are approved by the U.S. Food and Drug Administration for nausea and vomiting in pregnancy. Ginger may be used as a nonpharmacologic option to reduce symptoms. A meta-analysis of 13 RCTs found that ginger more effectively relieves nausea compared with placebo, but has similar relief to vitamin B6; however, there was no significant effect on vomiting.43 Several common antiemetics such as diphenhydramine, promethazine, and ondansetron may be used for persistent symptoms, although evidence for safety and effectiveness is limited.21,28 For hyperemesis gravidarum, corticosteroids are effective in refractory cases but should be the last option before 10 weeks of gestation because they are associated with the development of oral clefts in infants.
OTHER THERAPIES
Complementary and alternative therapies are increasingly being used for nausea and vomiting.30 Ginger is thought to be a serotonin antagonist and has antispasmodic effects in the GI tract.28,29 There is evidence to support the use of ginger for acute migraine.29,44 A recent meta-analysis of RCTs found medical cannabinoids, including dronabinol and nabilone (Cesamet), to be helpful for nausea and vomiting, primarily in the setting of cancer, but they were not more effective than placebo in some studies.45 Additionally, evidence supporting the use of other forms of cannabis to treat nausea and vomiting is lacking.30
This article updates previous articles on this topic by Anderson and Strayer4 and Scorza, et al.13
Data Sources: A PubMed search was completed using the key terms nausea and vomiting. The Cochrane database, UpToDate, ACCESSSS, and Essential Evidence Plus were also searched. The search included meta-analyses, randomized controlled trials, reviews, and clinical practice guidelines. Our review did not incorporate race or gender as patient categories. Search dates: April 2023, May 2023, and March 2024.
